


















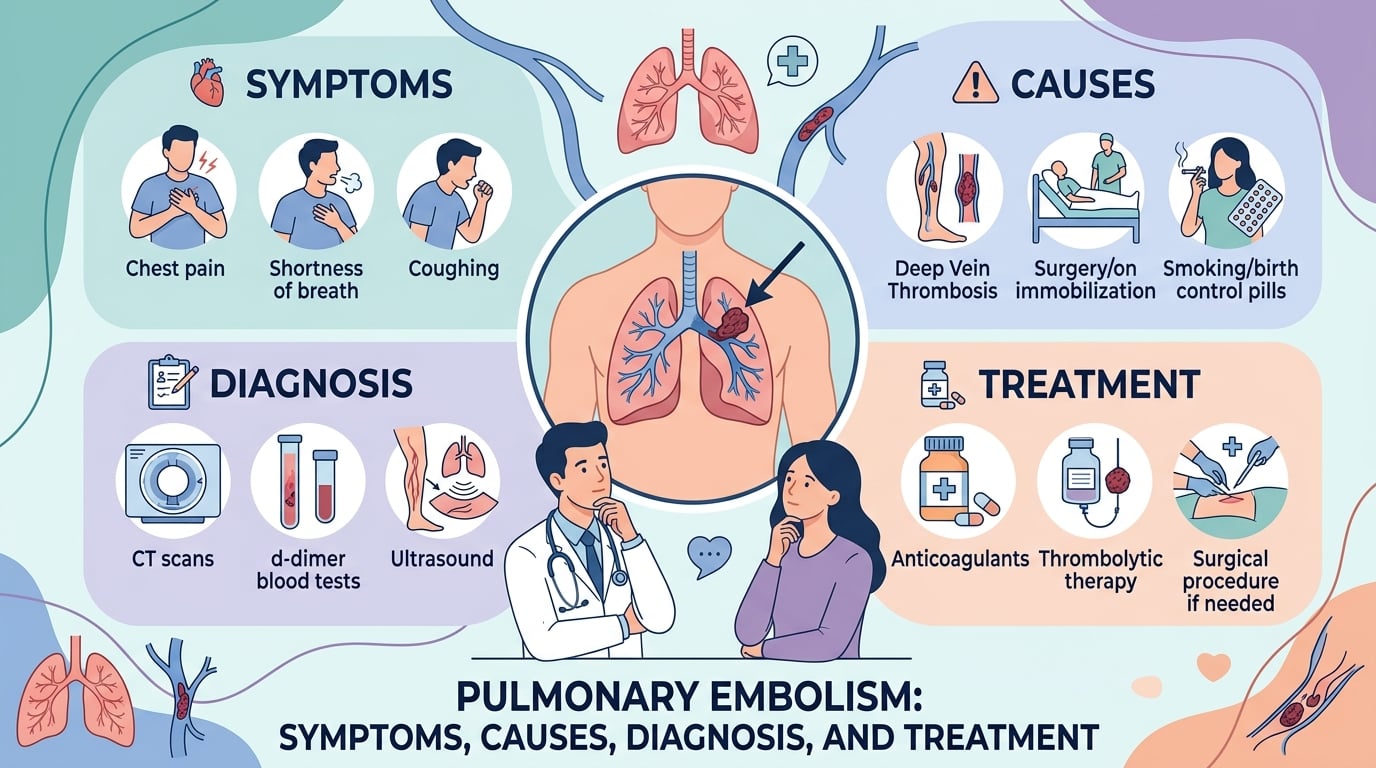
A pulmonary embolism is a blood clot that blocks one of the arteries in your lungs, usually after a clot in a deep vein of the leg breaks loose and travels upward. It can range from mild to life-threatening, and the warning signs — sudden shortness of breath, sharp chest pain, a racing heartbeat — are easy to mistake for other problems. This article explains, in plain language, what a pulmonary embolism is, what causes it, and who is most at risk. You will also learn how doctors use a D-dimer blood test, a CT scan, and cardiac markers to diagnose and grade it, what the main treatments involve, and what recent research is changing. Throughout, the goal is clear, calm information — not a substitute for medical care.
What is a pulmonary embolism?
A pulmonary embolism, often shortened to PE, happens when a clump of material — almost always a blood clot — lodges in a pulmonary artery, one of the vessels that carry blood from the heart to the lungs. Most clots start as a deep vein thrombosis (DVT), usually in the calf or thigh. A piece can break away, travel through the right side of the heart, and become stuck where the lung’s blood vessels narrow.
When blood cannot pass freely, two things happen. The affected part of the lung receives less blood flow, so the body struggles to add oxygen to the blood. At the same time, the right side of the heart has to push harder against the blockage, which can strain it. A large or sudden blockage is what turns some cases into an emergency.
A clot in a lung artery is a venous problem, and it behaves differently from the arterial clots behind a heart attack or stroke; to compare the two conditions, see our guide to stroke (cerebrovascular accident).
Symptoms and warning signs of a pulmonary embolism
Symptoms vary with the size of the clot and your overall health. Some people feel dramatically unwell within minutes; others have only vague, on-and-off symptoms. Common signs include:
- Sudden shortness of breath, even at rest, that often worsens with activity
- Sharp chest pain that gets worse when you breathe deeply, cough, or bend over
- A fast heart rate or a sense of your heart pounding
- Coughing, sometimes bringing up blood-streaked mucus
- Lightheadedness, fainting, or feeling like you might pass out
- Pain, swelling, warmth, or redness in one leg, a sign of the original DVT
Because these symptoms overlap with pneumonia, a panic attack, or a heart problem, a pulmonary embolism is easy to miss. That is also why people often ask how long a clot can sit silently in the lungs: small clots can cause little more than mild breathlessness for days. The safe response is never to wait it out.
Warning signs that need emergency care
Call your local emergency number (911 in the United States) right away if you or someone near you has:
- Sudden, severe shortness of breath
- Chest pain that does not ease, especially with fainting
- Coughing up blood
- A fast or irregular heartbeat with dizziness, blue-tinged lips, or collapse
In a minority of cases the first sign is sudden collapse, which is the main reason clinicians urge people not to delay. According to the CDC, sudden death is the first symptom in about 1 in 4 people who have a pulmonary embolism — a sobering figure that is also a strong argument for acting fast rather than panicking.
What causes a pulmonary embolism?
Nearly all pulmonary embolisms begin with a blood clot in a deep vein, so the causes of PE are largely the causes of DVT. Doctors group the underlying drivers into what is known as Virchow’s triad: slow or pooling blood flow, injury to a vein wall, and blood that clots too easily.
On top of those mechanisms, several situations raise the risk:
- Long periods of not moving — major surgery, hospital stays, bed rest, a leg cast, or long flights and car trips
- Recent surgery or a serious injury, especially to the hips, knees, or pelvis
- Cancer and some cancer treatments
- Pregnancy and the weeks just after giving birth
- Estrogen-containing birth control or hormone therapy
- Inherited or acquired clotting disorders (thrombophilia)
- Older age, obesity, smoking, and previous clots
Cancer is one of the strongest triggers, partly because some tumors and treatments make the blood more likely to clot; to learn more about one example, see our guide to lung cancer.
Some clotting tendencies run in families, while others are acquired, including a raised level of an amino acid called homocysteine; for the blood test that measures it, see our guide to homocysteine levels.
Long-standing heart and lung conditions add to the risk as well; for one common example, see our guide to heart failure.
How is a pulmonary embolism diagnosed?
No single symptom proves a pulmonary embolism, so doctors combine a risk assessment, blood tests, and imaging. The order of steps depends on how unwell you are and how likely a clot seems.
Clinical assessment and the Wells score
For stable patients, clinicians often begin by estimating the probability of a clot. A widely used tool, the Wells score, adds points for factors such as signs of a leg clot, a heart rate above 100, recent surgery or immobility, a previous clot, coughing up blood, and active cancer. The total sorts people into lower or higher probability, which decides whether a simple blood test is enough or imaging is needed next.
The D-dimer blood test
D-dimer is a small protein fragment released when the body breaks down a blood clot. A pulmonary embolism usually raises it, so the test is sensitive. The catch is that it is not specific: infection, recent surgery, pregnancy, and even older age can lift D-dimer too. Because of this, a normal D-dimer in someone at low risk is reassuring and can help avoid a scan, while a high result is a prompt for imaging rather than a diagnosis on its own.
On a lab report, the D-dimer often appears next to other clotting values; to understand the full panel, see our guide to the coagulation panel.
Imaging tests
Imaging confirms or rules out the clot. The standard test is a CT pulmonary angiography (CTPA), a CT scan with contrast dye that shows the lung arteries directly; the CDC describes CTPA as the standard imaging test for PE. When a CT scan is not suitable — for example, in pregnancy or with certain dye allergies — a ventilation–perfusion (V/Q) scan is an alternative. An ultrasound of the leg veins can also reveal the source clot.
Blood tests that gauge severity
Once a pulmonary embolism is confirmed, other blood tests help judge how much strain it is putting on the heart. A rise in troponin can signal that the heart’s right chamber is under pressure; to read what this protein means, see our guide to troponin. Doctors may also check BNP or NT-proBNP, hormones the heart releases when it is stretched; for more, see our guide to BNP. These heart-related tests are usually ordered together, often with an ECG; to see how they fit, read our guide to the cardiac markers panel. Baseline bloods such as kidney function and a blood count are drawn at the same time; to read yours, see our guide to the complete blood count. Lab reports can be hard to decode; for a plain-language walkthrough, see our guide to reading blood test results.
Tests used to evaluate a suspected pulmonary embolism
| Test | What it measures | How it helps |
|---|---|---|
| Wells score | Clinical risk factors | Estimates how likely a clot is and guides next steps |
| D-dimer | Clot-breakdown fragments in the blood | Helps rule out a clot in lower-risk people |
| CT pulmonary angiography (CTPA) | A direct image of the lung arteries | Confirms or excludes the clot (standard test) |
| Ventilation–perfusion (V/Q) scan | Air flow versus blood flow in the lungs | An alternative when a CT scan is not suitable |
| Leg vein ultrasound | Clots in the deep leg veins | Finds the likely source (DVT) |
| Troponin and BNP | Strain on the heart | Grade severity and guide treatment |
How is a pulmonary embolism treated?
Treatment has two goals: stop the existing clot from growing and prevent new ones, then, in severe cases, remove or dissolve the blockage quickly.
Anticoagulants (blood thinners)
For most people, anticoagulants are the mainstay. These medicines do not melt the clot; they stop it from enlarging and let the body break it down over time. The CDC notes that anticoagulants are the most common treatment for DVT and PE. Options include direct oral anticoagulants (DOACs) taken as tablets, injectable heparins, and warfarin.
Warfarin needs regular blood tests to keep it in a safe range, reported as the PT/INR; to understand this value, see our guide to vitamin K and the PT/INR test.
Clot-dissolving and clot-removing treatments
When a pulmonary embolism causes dangerously low blood pressure (high-risk PE), doctors may use clot-dissolving drugs called thrombolytics, given through a vein. For selected patients, a catheter can deliver these drugs directly to the clot or physically remove it, a procedure called thrombectomy. In rare, severe cases, surgery is considered. These approaches carry a higher bleeding risk, so they are reserved for the most serious situations.
How long treatment lasts
Most people take anticoagulants for at least three months. If the clot followed a temporary trigger such as surgery, treatment may stop after that. If the cause was unprovoked or ongoing — for example, certain cancers or clotting disorders — longer or indefinite treatment may be advised. Your doctor weighs the risk of another clot against the risk of bleeding.
Recovery, outlook, and prevention
Many people recover well from a pulmonary embolism, especially when it is found and treated promptly. Breathlessness and tiredness can linger for weeks to months as the lungs and heart recover. A minority develop chronic thromboembolic pulmonary hypertension, a lasting rise in lung-artery pressure that needs specialist care, which is one reason follow-up appointments matter.
You cannot prevent every clot, but you can lower your risk:
- Move regularly on long flights or drives, and after surgery or illness
- Stay active, manage your weight, and avoid smoking
- Take prescribed blood thinners exactly as directed
- Tell your care team about past clots or a family history before any surgery
- Stay hydrated and use compression stockings if your doctor recommends them
If you have already had a clot, recognizing the early signs of a new one — and acting fast — is one of the most useful things you can do.
Latest scientific advances
For most people with a pulmonary embolism, blood thinners remain the standard first-line treatment, and that has not changed. Research indexed in PubMed maps where care is evolving. A 2025 review of contemporary PE management notes that systemic clot-dissolving drugs are first-line only for high-risk PE with unstable blood pressure, while anticoagulation alone remains standard for stable “intermediate-risk” patients — though that group still carries meaningful risk, which is why newer catheter techniques are being studied (Guarnieri et al., International Journal of Cardiology, 2025; DOI).
One key question is whether removing or dissolving the clot through a catheter, on top of blood thinners, helps people whose right heart is strained but whose blood pressure is still normal (intermediate-high-risk PE). The STORM-PE trial — the first randomized controlled trial (a study in which patients are assigned by chance, for a fair comparison) of catheter-based clot suction plus anticoagulation versus anticoagulation alone — followed 100 patients. The suction group had a larger, faster drop in a heart-strain measure at 48 hours and quicker normalization of vital signs, with serious complication rates similar to blood thinners alone. Importantly, this was a small trial that measured a short-term imaging marker rather than survival, and two PE-related deaths occurred in the catheter group — so the results are promising but not proof of a survival benefit (Lookstein et al., Circulation, 2025; DOI).
A larger 2024 trial, PEERLESS, compared two catheter techniques against each other — large-bore mechanical clot removal versus catheter-delivered clot-dissolving drugs — in 550 intermediate-risk patients. Clot removal was linked to fewer episodes of clinical worsening and far less intensive-care use, with no difference in death or major bleeding. This trial compared two procedures, not a procedure against blood thinners alone (Jaber et al., Circulation, 2024; DOI).
Specialist groups urge caution. The 2025 European Society of Vascular Medicine guideline on catheter-based treatment of clots stresses that these procedures should be reserved for selected patients, chosen by an experienced team, and performed in specialized centers (Schlager et al., Vasa, 2025; DOI). In short, catheter treatments are an active and promising area, mainly for more severe intermediate-risk cases — but for the typical patient, blood thinners remain the foundation of care.
Recent research at a glance
| Recent study (year) | Type | Main finding | What it means |
|---|---|---|---|
| STORM-PE (2025) | Randomized trial, 100 patients | Catheter clot suction plus blood thinners eased heart strain faster than blood thinners alone | Promising for intermediate-high-risk PE; a short-term marker, not survival |
| PEERLESS (2024) | Randomized trial, 550 patients | Mechanical clot removal caused less clinical worsening and less ICU use than catheter clot-dissolving drugs | Compares two procedures, not procedure versus blood thinners |
| Contemporary management review (2025) | Review | Anticoagulation stays standard for stable PE; reperfusion reserved for severe cases | Frames where newer options fit |
| ESVM guideline (2025) | Practice guideline | Catheter treatments for selected patients in expert centers | Newer is not automatically better for everyone |
Glossary
| Term | Definition |
|---|---|
| Anticoagulant | A medicine that slows blood clotting to stop a clot from growing and prevent new ones; often called a blood thinner. |
| CT pulmonary angiography (CTPA) | A CT scan with contrast dye that shows the lung arteries; the standard imaging test for a pulmonary embolism. |
| D-dimer | A protein fragment released when the body breaks down a clot; a blood test used to help rule out clots. |
| Deep vein thrombosis (DVT) | A blood clot in a deep vein, most often in the leg, that can travel to the lungs. |
| Embolus | A clot or other material that travels through the bloodstream and lodges in a vessel elsewhere. |
| Pulmonary embolism (PE) | A blood clot blocking an artery in the lungs. |
| Right ventricular strain | Extra pressure on the heart’s right pumping chamber, used to judge how serious a clot is. |
| Thrombectomy | A procedure that physically removes a clot from a blood vessel. |
| Thrombolytic | A clot-dissolving medicine used in severe cases. |
| Venous thromboembolism (VTE) | The umbrella term covering both deep vein thrombosis and pulmonary embolism. |
Frequently asked questions
How long can you have a pulmonary embolism without knowing?
It varies. A small clot may cause only mild, on-and-off breathlessness or a slightly fast heartbeat, and some clots are found by chance during a scan for another reason. Larger clots usually cause clear, sudden symptoms. Because there is no reliable way to judge the size from how you feel, clinicians advise against waiting: if you have unexplained shortness of breath, chest pain, or a swollen, painful leg, get checked promptly rather than assuming a clot is small.
What does a pulmonary embolism feel like?
The classic feeling is sudden shortness of breath that does not improve with rest, often with a sharp chest pain that worsens when you breathe in. Many people also notice a racing heart, lightheadedness, or anxiety, and some have leg pain or swelling from the original clot. Symptoms can be milder, though, which is part of what makes a pulmonary embolism tricky. Any sudden, unexplained breathing difficulty deserves urgent medical attention.
Can you survive a pulmonary embolism?
Yes. Many people survive and recover well, particularly when the clot is recognized and treated quickly. The outlook depends on the size of the clot, how fast treatment begins, and your overall health, including conditions such as cancer or heart disease. Severe clots can be dangerous, which is why speed matters, but a pulmonary embolism is not automatically fatal — prompt blood thinners and good follow-up give most people a strong chance of recovery.
Does a D-dimer test confirm a pulmonary embolism?
No. A D-dimer test measures fragments left when the body breaks down clots, so it is sensitive but not specific. In someone at low risk, a normal D-dimer is reassuring and can help avoid a scan. A high D-dimer, however, can come from infection, recent surgery, pregnancy, or simply older age, so it does not confirm a clot on its own — imaging such as a CT scan is needed for that.
How can I lower my risk of a pulmonary embolism?
Keep moving during long flights, car trips, and after surgery or illness; even short stretches help. Stay active, manage your weight, and avoid smoking. If you are prescribed blood thinners, take them exactly as directed, and tell your care team about any past clots or a family history before an operation. People at higher risk during hospital stays are often given preventive measures, so it is worth asking your doctor what applies to you.
Can a pulmonary embolism go away on its own?
The body can slowly dissolve small clots, but a pulmonary embolism still needs medical treatment. Without blood thinners, a clot can grow, a new one can form, or strain on the heart can worsen, sometimes quickly. Treatment lowers these risks and supports recovery. So while clots do break down over time, this is not a reason to delay care; a suspected clot should always be assessed by a clinician.
Sources
- Pulmonary embolism — Symptoms and causes (Mayo Clinic)
- About Venous Thromboembolism / blood clots (CDC)
- Pulmonary Embolism (Cleveland Clinic)
- Guarnieri et al., Contemporary management of acute pulmonary embolism, International Journal of Cardiology, 2025 (PubMed) — DOI
- Lookstein et al., STORM-PE randomized trial, Circulation, 2025 (PubMed) — DOI
- Jaber et al., PEERLESS randomized trial, Circulation, 2024 (PubMed) — DOI
- Schlager et al., 2025 ESVM Guidelines on interventional treatment of VTE, Vasa, 2025 (PubMed) — DOI
Further reading
- Coagulation panel: PT, PTT, INR and D-dimer
- Cardiac markers: troponin, BNP and CK
- Heart failure: understanding and managing it
- Stroke (cerebrovascular accident)
- How to read your blood test results
Understand your lab results with AI DiagMe
If a clot was suspected or treated, you may leave the clinic with several lab results to make sense of — a D-dimer, cardiac markers such as troponin and BNP, and clotting values like the PT/INR. AI DiagMe helps you understand what those numbers mean in plain language, drawing on an analysis reviewed by a panel of physicians. It does not diagnose disease or replace your doctor, but it can help you walk into your next appointment with clearer questions.
➡️ Get your results interpreted in minutes
{kind=link}