


















Cardiac markers are substances your heart releases into the blood when it is stressed or damaged. When you have chest pain or shortness of breath, doctors often order a cardiac marker panel — most commonly troponin, BNP, and creatine kinase (CK) — to check how your heart is doing. Seeing these names on a lab report can be confusing, especially when a value is flagged as high. This guide explains, in plain language, what each of these three blood tests measures, what normal and elevated results usually mean, why a doctor orders them, and which warning signs need urgent care. You will also find a comparison table, a glossary, and answers to the questions patients ask most. The goal is to help you understand your results and have a more informed conversation with your doctor.
What are cardiac markers?
Cardiac markers (also called cardiac biomarkers) are proteins and enzymes that leak into your bloodstream when heart muscle is injured or under strain. A healthy heart releases very little of them, so when blood levels climb, it can signal that something is affecting the heart. Measuring them with a simple blood test gives doctors a fast, low-cost clue about what is happening inside your chest, which is one reason it helps to understand how to read a blood test report before your appointment.
The three markers used most often today are troponin, BNP (a heart hormone), and creatine kinase (CK), an enzyme. Older or supporting markers such as myoglobin and LDH (lactate dehydrogenase) are sometimes measured too, but they have largely been replaced by troponin for diagnosing a heart attack. Each marker tells a slightly different story, which is why doctors often look at several together rather than relying on one number.
The three main cardiac markers
A cardiac marker panel usually combines tests that answer different questions. Is the heart muscle being damaged right now? Is the heart under pressure or failing? Is muscle anywhere in the body breaking down? Here is what each of the three main markers measures.
Troponin: the marker for heart muscle damage
Troponin is a protein found inside heart muscle cells. When those cells are damaged — most importantly during a heart attack (myocardial infarction) — troponin spills into the blood. Because the heart uses its own version of this protein, a raised troponin level points fairly specifically to heart injury. This specificity is why troponin is now the preferred blood test for diagnosing a heart attack, replacing older enzyme tests.
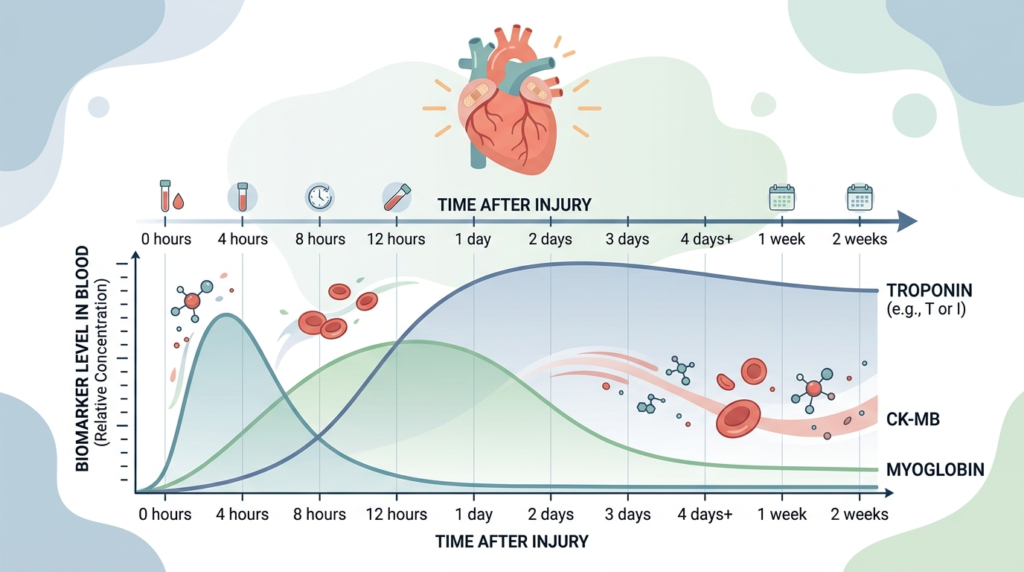
Modern laboratories use high-sensitivity troponin tests that can detect very small amounts within a few hours of injury. Levels typically rise within one to three hours, peak over the following day, and can stay elevated for up to about two weeks. A single result is rarely enough on its own. Doctors usually repeat the test a few hours later to see whether the level is rising or falling, which helps separate a new heart attack from a stable, long-standing elevation.
BNP and NT-proBNP: markers of heart strain and heart failure
BNP stands for B-type natriuretic peptide, a hormone the heart releases when its chambers are stretched or working under extra pressure. The more the heart is strained, the more BNP it produces. For that reason, BNP and a closely related fragment called NT-proBNP are used mainly to help diagnose and monitor heart failure, a condition in which the heart cannot pump blood as well as it should.
A high BNP level supports the diagnosis of heart failure and can reflect how severe it is, while a normal level makes heart failure unlikely as the cause of symptoms such as breathlessness or swollen ankles. BNP values naturally rise with age and reduced kidney function, and they tend to be lower in people with obesity. Doctors therefore interpret the number alongside your overall picture rather than on its own.
Creatine kinase (CK) and CK-MB: muscle and heart enzymes
Creatine kinase is an enzyme found in muscle tissue throughout the body, including the heart. When muscle is damaged, creatine phosphokinase (CPK) — the full name for total CK — is released into the blood. Total CK is not heart-specific. It can rise after intense exercise, a fall, an injection, or a muscle disorder, so a high total CK does not by itself mean a heart problem.
To look specifically at the heart, laboratories can measure CK-MB, the fraction of creatine kinase that comes mostly from heart muscle. CK-MB was once a standard test for heart attacks, but troponin has largely taken over because it is more sensitive and more specific. Today, total CK is most useful for muscle-related conditions — for example, suspected rhabdomyolysis (severe muscle breakdown) or muscle side effects from certain medicines — rather than for diagnosing a heart attack.
Cardiac markers at a glance: a comparison
Because each marker behaves differently, a quick side-by-side view helps. The table below summarizes what each cardiac marker measures, what a rise usually suggests, and how the timing differs. Reference ranges depend on the laboratory and the testing method, so always read your own report’s stated range.
| Marker | What it measures | Mainly used for | Typical timing of a rise |
|---|---|---|---|
| Troponin (cTnI, cTnT) | A protein specific to heart muscle | Diagnosing a heart attack and other heart-muscle injury | Rises within about 1–3 hours, peaks within roughly a day, can stay high up to about 2 weeks |
| BNP / NT-proBNP | A hormone released when the heart is under pressure | Diagnosing and monitoring heart failure | Reflects ongoing strain; changes over days as the condition changes |
| Creatine kinase (CK / CPK) | An enzyme from muscle anywhere in the body | Muscle damage, such as rhabdomyolysis or medicine-related injury | Rises within hours, can peak about 1–2 days after muscle injury |
| CK-MB | The heart-related fraction of CK | An older heart-attack marker, now mostly replaced by troponin | Rises within hours, returns to normal within about 2–3 days |
A practical takeaway: troponin answers “is the heart muscle being injured?”, BNP answers “is the heart under strain or failing?”, and CK answers “is muscle being damaged somewhere in the body?”.
What do your cardiac marker results mean?
Lab reports usually show your result next to a reference range — the values expected in people without the relevant condition. A result inside the range is reported as normal, and a value above it is flagged high, often with an “H”. A flagged value is not the same as a dangerous one, though: with cardiac markers, the trend over time and your symptoms matter as much as a single number.
Reading troponin results
For high-sensitivity troponin, many laboratories use a cutoff based on the 99th percentile of a healthy population, sometimes with separate thresholds for men and women. A level below the cutoff is reassuring. A clearly raised level, or a level that rises significantly between two tests, suggests heart-muscle injury. A mildly raised but stable value can have many causes other than a heart attack, which is why doctors look at the pattern rather than one reading.
Reading BNP and NT-proBNP results
A low BNP or NT-proBNP makes heart failure an unlikely explanation for breathlessness, while higher values increase the likelihood and can track severity. Because age, kidney function, and body weight shift the numbers, the same value can mean different things in different people. Your doctor compares the result with your symptoms, a physical examination, and often an ultrasound scan of the heart.
Reading CK results
A raised total CK signals muscle damage somewhere, not necessarily the heart. Very high levels can point to rhabdomyolysis, which can affect the kidneys and needs prompt attention. If a heart problem is the concern, troponin — not CK — is the test that settles it. Intense exercise in the days before the test is a common and harmless reason for a higher CK reading.
Why a doctor orders a cardiac marker panel
The most common reason is to investigate symptoms that could come from the heart, especially chest pain or shortness of breath. In an emergency department, troponin is measured quickly, and often repeated, to confirm or rule out a heart attack. BNP or NT-proBNP may be added when heart failure is suspected, for example in someone with breathlessness and swollen legs.
Doctors also use these tests to monitor a known heart condition over time, to check the heart after certain surgeries or procedures, and as part of a broader work-up. When the cause of chest pain or breathlessness is unclear, other blood tests may be ordered alongside them — for instance a D-dimer to help assess the chance of a blood clot in the lungs, or an inflammation marker such as CRP (C-reactive protein). None of these tests is used alone; each adds a piece to the picture.
When cardiac markers rise without a heart attack
One of the most common worries is a raised troponin without a heart attack. It is important to know that troponin can be elevated for many reasons besides a blocked artery. Any condition that stresses or injures the heart, or that slows the clearance of troponin from the body, can lift the level.
Common non-heart-attack causes of a raised troponin include:
- Reduced kidney function, which slows how troponin is cleared from the body — this is why creatinine, a kidney marker, is often checked alongside it
- Severe infections or critical illness, such as sepsis
- A fast or irregular heartbeat, or very high blood pressure
- Heart failure, myocarditis (inflammation of the heart muscle), or a pulmonary embolism (a clot in the lungs)
- Strenuous endurance exercise in some people
The same logic applies to CK, which rises with ordinary muscle activity or injury, and to BNP, which climbs with age and kidney problems. This is exactly why a single high value is not a diagnosis. Doctors interpret cardiac markers together with your symptoms, your other test results, and how the numbers change over time.
Warning signs that need urgent care
A blood test cannot replace acting quickly when symptoms suggest a heart attack. Cardiac markers take time to be drawn and processed, so the decision to seek emergency help should be based on symptoms, not on waiting for a number.
Call your local emergency number (such as 911 in the United States) right away if you or someone else has:
- Chest pain, pressure, tightness, or squeezing that lasts more than a few minutes or comes and goes
- Pain spreading to the arm, shoulder, neck, jaw, or back
- Sudden shortness of breath, with or without chest discomfort
- Cold sweat, nausea, or lightheadedness
- A strong sense that something is seriously wrong, alongside any of the above
Symptoms can be milder or different in women, older adults, and people with diabetes — for example, unusual fatigue, indigestion-like discomfort, or breathlessness without obvious chest pain. When in doubt, treat it as an emergency. Acting fast protects heart muscle.
How the test is done and what can affect results
A cardiac marker panel is a standard blood draw, usually from a vein in your arm, and it takes only a few minutes. In an emergency, the sample is processed quickly and often repeated after a few hours so the team can see whether troponin is rising. Many hospitals now use rapid pathways that compare two high-sensitivity troponin samples taken about one to three hours apart, which allows them to safely rule a heart attack in or out faster than older tests did. You usually do not need to fast for these tests, but follow whatever instructions your clinic gives, because they may be checking other markers at the same time.
Several everyday factors can nudge the numbers. Intense exercise in the previous day or two can raise CK and, in some people, troponin. Reduced kidney function can raise troponin and BNP. Age and body weight shift BNP. Certain medicines and recent procedures matter too. None of this means a result is “wrong” — it means the number has to be read in context. The most reliable interpretation comes from your doctor, who weighs the values against your history, your examination, and any heart imaging.
Glossary
- Acute coronary syndrome (ACS): An umbrella term for a sudden drop in blood flow to the heart, ranging from unstable chest pain to a heart attack.
- Biomarker: A measurable substance in the body, such as a protein or enzyme, that gives information about a health condition.
- BNP (B-type natriuretic peptide): A hormone released when the heart is under strain; used mainly to assess heart failure.
- CK-MB (creatine kinase-MB): The fraction of creatine kinase that comes mostly from heart muscle; an older heart-attack marker.
- Creatine kinase (CK): A muscle enzyme that rises in the blood when muscle anywhere in the body is damaged. Also written CPK.
- High-sensitivity troponin: A modern, very sensitive troponin test that can detect small amounts of the protein within a few hours of heart injury.
- Myocardial infarction: The medical term for a heart attack, when part of the heart muscle is damaged by a lack of blood flow.
- NT-proBNP: A protein fragment produced along with BNP; like BNP, it is used to help diagnose and monitor heart failure.
- Reference range: The span of values expected in people without the condition being tested; your result is compared against it.
- Troponin: A protein specific to heart muscle; a raised blood level is a key sign of heart-muscle injury.
Frequently asked questions
Can troponin be high without a heart attack?
Yes. A raised troponin means heart-muscle injury or stress, but a blocked artery is only one cause. Reduced kidney function, severe infections, heart failure, inflammation of the heart muscle, a clot in the lungs, a very fast heartbeat, and sometimes intense endurance exercise can all lift the level. This is why doctors rarely act on a single value. They look at whether it is rising or stable, at your symptoms, and at your other results. A mildly raised, unchanging troponin in someone without cardiac symptoms often reflects an ongoing condition rather than a new heart attack.
How long does troponin stay elevated after a heart attack?
After heart-muscle injury, troponin usually starts to rise within one to three hours, peaks over the following day, and can remain detectable for up to about two weeks. Because it stays up for so long, troponin can confirm a recent heart attack even if you did not seek care immediately. It also means doctors rely on the pattern of change between repeated tests, rather than one reading, to judge whether an injury is new and ongoing. Your own timeline depends on the size of the injury and your kidney function.
What is the difference between BNP and NT-proBNP?
Both come from the same precursor hormone that the heart makes when its walls are stretched. When that precursor is split, it produces active BNP and an inactive fragment called NT-proBNP. Laboratories may measure either one to assess heart failure; they carry similar information but use different reference ranges, so the two numbers are not interchangeable. NT-proBNP tends to stay in the blood longer and is affected more by kidney function and age. Your lab report will state which test was used and its expected range.
Can I lower my troponin or CK levels myself?
Cardiac markers are not numbers you treat directly; they are signals of what is happening underneath. Troponin reflects heart-muscle stress or injury, and CK reflects muscle damage, so the levels fall when the underlying cause is addressed, not through a quick fix. If a marker is raised, the useful step is to work with your doctor to find and manage the cause, whether that is a heart condition, a kidney issue, or recent strenuous exercise affecting CK. Never ignore a raised cardiac marker or try to “correct” it on your own.
Do I need to fast before a cardiac marker blood test?
Usually no. Troponin, BNP, and CK do not require fasting, and in an emergency the test is done immediately regardless of when you last ate. However, your doctor may check other markers at the same visit — for example cholesterol or blood sugar — that do need fasting. The safest approach is to follow the specific instructions your clinic gives you when the test is booked, and to mention any recent intense exercise, which can raise CK.
Are cardiac markers used to screen healthy people for heart disease?
Generally no. Troponin, BNP, and CK are mainly used to investigate symptoms or monitor a known condition, not to screen people who feel well. To estimate future heart-disease risk, doctors more often look at markers such as cholesterol, together with blood pressure, lifestyle, and family history. If you are concerned about your risk rather than current symptoms, a conversation about prevention and the right preventive tests — including a review of high cholesterol — is usually more useful than a cardiac marker panel.
Sources
- Cardiac Enzymes (Biomarkers) — Cleveland Clinic
- Troponin Test — MedlinePlus, U.S. National Library of Medicine
- Blood tests for heart disease — Mayo Clinic
Further reading
- Troponin: understanding this cardiac marker
- BNP: a key cardiac health marker
- Creatine Kinase-MB (CK-MB): understanding this cardiac marker
- Heart failure: understanding and managing it
- How to read your blood test results
Understand your lab results with AI DiagMe
A cardiac panel is rarely the only line on a lab report — your troponin, BNP, or creatine kinase (a muscle enzyme) often sit beside kidney, liver, and inflammation results. AI DiagMe helps you make sense of these numbers in plain language, putting each value in context so you arrive at your appointment better informed. It is built to support understanding, not to diagnose, and it never replaces your doctor’s judgment. If you have a recent blood test, you can get a clear, easy-to-read interpretation in just a few minutes.
➡️ Get your results interpreted in minutes
{kind=link}