


















A leukemia blood test is often the first clue that something is wrong with the body’s blood-forming system. Leukemia is a cancer of the blood and bone marrow, and because it usually does not create a lump you can see or feel, a simple blood sample becomes one of the most important tools doctors use to spot it. This article explains, in plain language, what leukemia is, the early signs to watch for, what a blood test can and cannot show, how a diagnosis is confirmed, and how treatment is changing. You will also find the latest research, a plain-English glossary, and clear guidance on when to talk to a doctor. Learning how to read the signals in your own results can help you ask sharper questions and feel more in control.
What leukemia is, and why blood tells the story
Leukemia begins in the bone marrow, the soft tissue inside your bones where blood cells are made. A single blood-forming cell develops a change in its DNA and starts to copy itself out of control. These abnormal cells, often immature white blood cells, crowd out the healthy red cells, white cells, and platelets your body needs.
Unlike most solid cancers, leukemia rarely forms a tumor that shows up on an X-ray or a scan. Instead, the disease lives in the blood and marrow. That is exactly why a blood sample is so revealing, and why so many people first hear the word leukemia after a routine lab result looks unusual. Learning to read your blood test results is a useful first step for anyone.
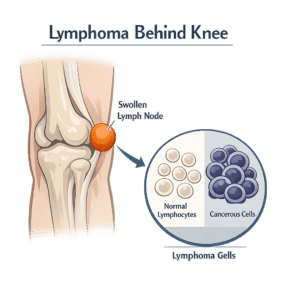
Leukemia is sometimes confused with lymphoma, another blood cancer. The simple difference: leukemia usually starts in the bone marrow and spills into the blood, while lymphoma usually starts in the lymph nodes and lymphatic system. The two can overlap, but they are diagnosed and treated differently.
The four main types of leukemia
Doctors sort leukemia along two lines. The first is speed: acute leukemias grow quickly and need prompt treatment, while chronic leukemias grow slowly and may be watched for years. The second is cell type: myeloid leukemias come from the cells that make red cells, platelets, and certain white cells, while lymphocytic leukemias come from lymphocytes, a type of infection-fighting white cell. Combining these gives four main types.
| Type | How fast it grows | Who it most often affects | A typical clue |
|---|---|---|---|
| Acute myeloid leukemia (AML) | Fast | Adults, risk rises with age | Low blood counts, immature cells (blasts) in the blood |
| Acute lymphoblastic leukemia (ALL) | Fast | The most common cancer in children | Blasts in the blood, often with bruising or infections |
| Chronic lymphocytic leukemia (CLL) | Slow | Older adults | A high lymphocyte count found on a routine test |
| Chronic myeloid leukemia (CML) | Slow | Mostly middle-aged and older adults | A high white cell count and a specific gene change |
There are rarer forms too, such as hairy cell leukemia. The type matters a great deal, because it shapes the symptoms, the blood findings, the treatment, and the outlook.
Early signs and symptoms to watch
Leukemia symptoms tend to be vague, and many of them look like everyday illnesses such as the flu. That is one reason early signs are easy to dismiss. The symptoms usually trace back to one problem: leukemia cells crowd out healthy blood cells, so the body runs short of what those cells normally do.
- Tiredness, weakness, or paleness, often from anemia (too few red cells).
- Frequent or hard-to-shake infections, because there are too few healthy infection-fighting white cells. A drop in these cells is called low absolute neutrophils.
- Easy bruising, small red or purple skin spots, bleeding gums, or frequent nosebleeds, often from a low platelet count. Unexplained marks can have many causes, including simple low iron and bruising.
- Bone or joint aches, fevers or drenching night sweats, swollen lymph nodes, or unexplained weight loss.
When the signs are subtle
Chronic leukemias can be quiet for a long time. Many people with CLL feel completely well, and the disease is found only because a routine blood draw shows a high lymphocyte count. As one Mayo Clinic specialist notes, most people with CLL are diagnosed by chance during a regular checkup, and only a minority have symptoms at first. None of these signs prove leukemia on their own, but a pattern that does not go away is worth checking.
What a leukemia blood test shows
The starting point is almost always a complete blood count, often shortened to CBC. This common test counts your red cells, white cells, and platelets, and it is the workhorse of a leukemia blood test. Several patterns can raise a doctor’s suspicion.
- White blood cell count that is too high, too low, or made up of unusual cells. A raised lymphocyte count, for example, is a hallmark of CLL; you can read more about high lymphocytes. Other leukemias can push the white cell count in either direction, sometimes with a rise in neutrophils, another type of white cell.
- Anemia, meaning a low red cell count or low hemoglobin, which often explains the fatigue and paleness.
- A low platelet count, which can explain easy bruising or bleeding.
- Immature cells called blasts appearing in the blood, where they normally should not be.
If the CBC looks suspicious, the lab usually examines a peripheral blood smear, a drop of blood viewed under a microscope, to see the size, shape, and maturity of the cells. Doctors also look at how counts change over time, since a single value matters less than a clear trend across repeated tests. Two other blood markers sometimes rise when cells are turning over quickly: lactate dehydrogenase (LDH) and uric acid. Neither is specific to leukemia, but together with the CBC they help build the picture.
It helps to know two limits of a blood test. First, leukemia is not found through the classic serum tumor markers used for some solid cancers; those proteins are not how blood cancers are detected. Second, a blood test can strongly suggest leukemia, but it cannot fully confirm it. Sometimes leukemia cells stay in the marrow and barely show in the blood, so a normal-looking CBC does not always rule the disease out. If the abbreviations on your own report look confusing, a short reference can help you match each code to what it measures.
How leukemia is diagnosed, beyond the blood test
A suspicious blood test opens an investigation rather than ending one. Confirming leukemia, and pinning down its exact type, usually follows a clear sequence.
- History and physical exam. A doctor asks about symptoms and checks for pale skin, swollen lymph nodes, or an enlarged spleen or liver.
- Blood tests. A CBC and a smear, plus follow-up tests on the same sample. If you have never had blood drawn, here is what the blood test process involves.
- Bone marrow test. A small sample of marrow, usually taken from the back of the hip bone, lets a specialist see how many abnormal cells are present.
- Flow cytometry and immunophenotyping. These tests read the proteins on the surface of the cells to identify exactly which kind of leukemia is present.
- Genetic and molecular tests. Cytogenetic and DNA-based tests look for the specific gene changes that guide treatment and predict how the disease may behave.
This is why an out-of-range blood result is a reason to look closer, not a diagnosis in itself. Most abnormal counts have causes far more common than cancer.
How leukemia is treated today
Treatment depends on the type of leukemia, the genetic features of the cells, and the person’s age and overall health. The main approaches include chemotherapy, targeted drugs that block specific gene changes, immunotherapy that turns the immune system against the cancer, and stem cell (bone marrow) transplant. For some slow-growing chronic leukemias, the right first step is active surveillance, sometimes called watch and wait, with regular checkups and blood tests rather than immediate treatment. Supportive care runs alongside these treatments and matters just as much: transfusions to correct low blood counts, antibiotics and other steps to prevent or treat infections, and medicines to ease side effects all help people get through therapy more safely.
Outlook varies widely. According to the National Cancer Institute, leukemia is most common in adults older than 55, yet it is also the most common cancer in children. Many childhood leukemias now have high long-term survival, while some adult forms remain serious and harder to treat. Numbers from large studies describe groups, not individuals, so they cannot predict any single person’s path.
Latest scientific advances
Few areas of cancer medicine have moved as fast as leukemia in recent years. The summary below draws on recent peer-reviewed reviews and consensus guidelines indexed on PubMed; full references and DOI links appear in the Sources section. Because these are expert syntheses rather than single experiments, they reflect where the field is heading, while still leaving room for ongoing study.
According to a 2025 update on AML from the Dana-Farber Cancer Institute, at least a dozen new therapies have been approved in the past decade, and risk is now graded using genetic and molecular features rather than appearance alone. A parallel 2025 update on adult ALL from MD Anderson describes how targeted drugs called tyrosine kinase inhibitors, used alone or with immunotherapy, have lifted five-year survival above 80 percent in a once high-risk subtype. Three themes stand out for patients.
- Targeted therapy. Drugs aimed at specific gene changes can be more precise, and sometimes gentler, than chemotherapy alone. They are already standard for CML and several AML and ALL subtypes. The same precision idea is reshaping related marrow conditions, such as SF3B1 myelodysplasia, a low-risk syndrome that can sometimes progress toward leukemia.
- Immunotherapy. CAR T-cell therapy, which re-engineers a patient’s own immune cells to hunt leukemia, has produced deep and often durable remissions. A 2026 review from the National Cancer Institute notes that since the first such therapy was approved in 2017, it has helped even complex cases of B-cell ALL, though roughly half of patients still relapse, so the approach keeps being refined. Antibody-based treatments are also changing standard care.
- Measurable residual disease (MRD). This means tiny traces of leukemia that remain after treatment and can only be found with very sensitive tests. A 2026 international consensus document published in the journal Blood describes how MRD results increasingly guide decisions, including whether a patient needs a stem cell transplant.
The table below sums up these directions.
| Advance | What it is | What it is changing | Where it stands |
|---|---|---|---|
| Targeted therapy | Drugs aimed at specific gene changes | More precise, sometimes gentler, treatment | Many drugs approved; standard in several subtypes |
| Immunotherapy | CAR T-cells and antibodies that direct the immune system at leukemia | Deep remissions in hard-to-treat B-cell leukemias | Approved for some B-cell ALL since 2017; expanding |
| MRD-guided care | Very sensitive testing for leftover leukemia | Helps decide who needs more treatment or a transplant | Increasingly built into guidelines and trials |
A word of caution fits here. A promising result in a clinical trial, which is a carefully run study in volunteers, is not the same as a proven cure, and some of these tools are still investigational or limited to certain subtypes. These advances are reasons for genuine optimism, not a do-it-yourself plan. Only a specialist can judge what fits a specific situation.
When to see a doctor
Most of the signs linked to leukemia turn out to have ordinary explanations, from a passing virus to low iron. Still, certain patterns deserve medical attention, especially when several appear together or last more than a couple of weeks.
- Unusual tiredness or breathlessness that does not improve with rest.
- Repeated infections, or a fever that keeps returning without a clear cause.
- Easy bruising, tiny red or purple skin spots, or bleeding that seems out of proportion to a minor injury.
- Drenching night sweats, unexplained weight loss, persistent bone pain, or swollen glands that do not settle.
The first step is usually simple: a doctor’s visit and a complete blood count. If a result comes back outside the normal range, that is a prompt to investigate calmly, not a verdict. Bringing your questions and your report to the appointment helps the conversation move faster.
Glossary
| Term | Definition |
|---|---|
| Acute leukemia | A fast-growing leukemia, made of immature cells, that usually needs prompt treatment. |
| Anemia | Too few red blood cells or too little hemoglobin, often causing tiredness and pale skin. |
| Blast cells | Very immature blood cells; finding many of them in the blood can point to acute leukemia. |
| Bone marrow | The soft tissue inside bones where blood cells are made. |
| Chronic leukemia | A slow-growing leukemia that may be watched for years before, or instead of, treatment. |
| Complete blood count (CBC) | A common blood test that counts red cells, white cells, and platelets. |
| Flow cytometry | A lab test that reads proteins on cells to identify the exact type of leukemia. |
| Lymphocyte | A type of white blood cell; a high count can be a sign of chronic lymphocytic leukemia. |
| Measurable residual disease (MRD) | Tiny traces of leukemia left after treatment, found only with very sensitive tests. |
| Platelets | Cell fragments that help blood clot; a low count can cause easy bruising or bleeding. |
Frequently asked questions
Can a routine blood test detect leukemia?
Often, yes. A complete blood count done for any reason can reveal patterns that suggest leukemia, such as an unusual white cell count, anemia, or a low platelet count. This is how many slow-growing leukemias are first found, in people who feel well. A routine test does not confirm the disease by itself, though. If the numbers look unusual, the doctor orders follow-up tests, which may include a blood smear and a bone marrow sample, to know for sure.
What does leukemia look like on a complete blood count?
There is no single picture, because it depends on the type. Common signals include a white cell count that is much too high or too low, a low red cell count or hemoglobin (anemia), and a low platelet count. In acute leukemias, the lab may also spot immature cells called blasts in the blood. None of these findings is proof on its own, since infections, medicines, and other conditions can move the same numbers.
Can you have leukemia with a normal blood test?
Sometimes. In certain cases, leukemia cells stay mostly in the bone marrow and barely appear in the bloodstream, so an early complete blood count can look close to normal. This is one reason doctors rely on symptoms, repeat testing, and a bone marrow sample when leukemia is suspected. A single normal result is reassuring, but it does not always rule the disease out if worrying symptoms continue.
Is leukemia curable?
It depends heavily on the type, the genetic features, and the person’s age and health. Some leukemias, especially in children, have high long-term survival, and many adults reach lasting remission. Other forms are harder to treat and are managed as long-term conditions. Treatments are improving quickly, including targeted drugs and immunotherapy. Survival statistics describe large groups, not individuals, so only a treating specialist can give a realistic outlook for a specific case.
What causes leukemia, and is it inherited?
In most cases the exact cause is unknown. Leukemia starts when blood-forming cells acquire DNA changes, and known factors that raise the risk include certain genetic conditions, past chemotherapy or radiation, heavy exposure to some chemicals, and tobacco smoke for some types. Most leukemia is not passed directly from parent to child, although a family history can slightly raise risk. Having a risk factor does not mean a person will develop the disease.
How long do leukemia blood test results take?
A basic complete blood count is often ready within hours to a day. The more detailed tests that confirm leukemia, such as flow cytometry, genetic studies, and a bone marrow review, usually take several days to come back, because they are more complex and are read by specialists. Waiting is hard, but these extra steps are what allow an accurate diagnosis and the right treatment plan.
Sources
- Leukemia: Symptoms and causes — Mayo Clinic
- Leukemia — Patient Version — National Cancer Institute (NIH)
- Leukemia: Symptoms, Causes, Types and Treatment — Cleveland Clinic
Recent peer-reviewed research (indexed on PubMed):
- Shimony S, Stahl M, Stone RM — Acute Myeloid Leukemia: 2025 Update on Diagnosis, Risk-Stratification, and Management (American Journal of Hematology, 2025)
- Kantarjian H, Jabbour E — Adult Acute Lymphoblastic Leukemia: 2025 Update on Diagnosis, Therapy, and Monitoring (American Journal of Hematology, 2025)
- Dreyzin A, et al. — The evolving landscape of CAR T cell therapy in children and young adults with B cell acute lymphoblastic leukemia (Molecular Therapy: Oncology, 2026)
- Cloos J, et al. — 2025 update on MRD in acute myeloid leukemia: a consensus document from the ELN-DAVID MRD Working Party (Blood, 2026)
Further reading
- Complete Blood Count (CBC): How to Read Your Results
- How to Read Your Blood Test Results
- High Lymphocytes: Causes, Symptoms, Treatments
- Lymphoma: Symptoms, Causes, and Treatments
- Common Medical Lab Test Abbreviations: A Guide
Understand your lab results with AI DiagMe
If you have just received a blood report and a value looks off, you do not have to decode it alone. AI DiagMe helps you understand what tests like a complete blood count (CBC), your white blood cell count, LDH, and uric acid actually measure, and what an out-of-range result may mean in plain language. It is built to help you make sense of your results and prepare for your appointment, not to diagnose you or replace your doctor.
➡️ Get your results interpreted in minutes

{kind=link}