


















A serology test is a blood test that looks for antibodies or antigens — the proteins your immune system makes, or the pieces of a germ — that show whether you have met a particular infection. On an STI and infectious disease panel, serology is the part that screens for infections such as HIV, syphilis, and hepatitis from a small blood sample. This guide explains, in plain language, what a serology test measures, how it differs from the urine and swab tests on the same panel, and how to make sense of words like “reactive,” “non-reactive,” and “titer.” You will also learn why timing changes your result, when a result needs a second confirming test, and when it is worth seeing a clinician. The goal is to help you read your own report with more confidence — not to replace advice from a healthcare professional.
What a serology test is (and what it measures)
A serology test examines a blood sample for signs of your body’s reaction to an infection. Rather than looking at the whole germ directly, it reads the immune “fingerprint” an infection leaves behind. Because antibodies can stay in the blood long after an infection begins — and sometimes for life — serology can reveal both current and past exposure.
A related part of a routine workup, the complete blood count, can show general signs that your body is fighting something, such as a change in white blood cells, and a marker like CRP reflects inflammation. A serology test is more specific: it names the germ your body has responded to.
Two ideas explain most of what a serology result is telling you.
Antibodies and antigens: what your blood is being checked for
- Antibodies are proteins your immune system makes to recognize a specific germ. Their presence usually means your body has encountered that germ, through infection or sometimes vaccination.
- Antigens are parts of the germ itself, such as the p24 antigen in HIV or the surface antigen in hepatitis B. Finding an antigen points more directly to the infection being present right now.
Many modern tests look for both at once. The standard HIV test, for example, is a combined “antigen/antibody” test, which lets it pick up an infection sooner than antibodies alone would allow.
IgM and IgG: timing clues in the result
Your report may mention two antibody types. IgM antibodies tend to appear first, in the early weeks of an infection. IgG antibodies appear a little later and often persist, marking a past or resolved infection or, for some germs, longer-term protection. Seeing IgM, IgG, or both helps a clinician estimate whether an infection is recent or older. For everyday screening you do not need to memorize these patterns — the laboratory and your clinician interpret them for you.
Where a serology test fits in an STI and infectious disease panel
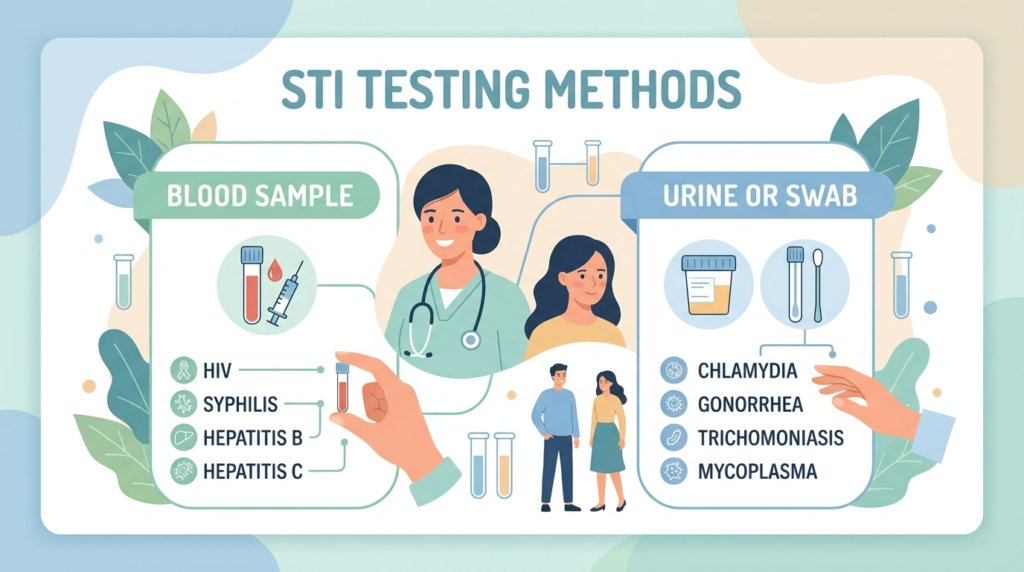
An STI or infectious disease panel is simply a group of tests ordered together so several infections can be checked in one visit. Most panels combine two kinds of samples: blood, which is used for serology, and urine or a swab, which is used for tests that look for a germ’s genetic material. Knowing which test uses which sample makes your results far easier to follow.
- Blood (serology) is standard for HIV, syphilis, hepatitis B, and hepatitis C, and sometimes herpes (HSV). These infections trigger an antibody or antigen response that a blood test can detect.
- Urine or swab (NAAT) is standard for chlamydia, gonorrhea, and trichomoniasis. These tests find the germ’s DNA directly rather than your antibodies. Infections such as ureaplasma and HPV are also detected this way, not by serology.
This is why a single appointment can involve both a blood draw and a urine sample or swab. A comparison of common blood panels follows the same logic: different panels group different tests for different jobs. During pregnancy, a similar prenatal blood panel screens for several of these infections to protect both parent and baby.
The table below summarizes what the most common panel tests look for, the sample each uses, and roughly how long after exposure each becomes detectable.
| Test (infection) | Sample type | What it detects | Typical time to become detectable* |
|---|---|---|---|
| HIV (antigen/antibody) | Blood (serology) | p24 antigen plus HIV antibodies | About 18–45 days for a lab test; antibody-only or self-tests up to about 90 days |
| Syphilis (RPR and treponemal) | Blood (serology) | Antibodies to the syphilis bacterium | About 3–6 weeks, sometimes up to about 12 weeks |
| Hepatitis B (HBsAg) | Blood (serology) | Hepatitis B surface antigen | About 3–6 weeks, up to a few months |
| Hepatitis C (anti-HCV) | Blood (serology) | Hepatitis C antibodies | About 8–11 weeks, up to about 6 months |
| Herpes (HSV IgG) | Blood (serology) | Herpes antibodies (not routine for everyone) | About 3–6 weeks, up to about 12–16 weeks |
| Chlamydia | Urine or swab (NAAT) | Chlamydia DNA (not serology) | About 1–2 weeks |
| Gonorrhea | Urine or swab (NAAT) | Gonorrhea DNA (not serology) | About 1–2 weeks |
| Trichomoniasis | Urine or swab (NAAT) | Trichomonas DNA (not serology) | About 1–2 weeks |
*These windows are general and vary by the specific test, the laboratory, and the individual. Your clinician advises on the best timing and whether a repeat test is needed.
How to read your serology test results: reactive, non-reactive, and titers
Serology results often use different words than the urine and swab tests on the same report. Here is what the common terms mean.
- Non-reactive (or negative): the blood did not show the antibody or antigen the test looks for. For most people this is reassuring, but it can be falsely reassuring if you tested during the window period (explained below).
- Reactive (or positive): the test found evidence of an immune response or an antigen. This is a signal to look closer, not always a final diagnosis.
- Equivocal or indeterminate: the result is borderline and usually needs repeating.
For swab and urine tests you are more likely to see “negative” or “not detected.” These carry the same meaning — no germ found — but use the wording typical of those methods. Our guide to reading blood test results explains more about how reports are laid out.
Why “reactive” does not always mean infected
A single reactive screening result is often only the first step. Screening tests are built to be very sensitive, so they occasionally flag people who are not infected — a false positive. That is why many infections use a two-step approach:
- HIV: a reactive screening test is followed by a separate confirmatory test before any diagnosis is made.
- Syphilis: laboratories combine a treponemal test (antibodies specific to the bacterium) with a non-treponemal test such as RPR, which is reported as a titer — a number like 1:8. The titer helps separate an active infection from a past, treated one and is used to track the response to treatment.
A titer is simply how far the blood can be diluted while still reacting; a higher number means more antibody. Watching a titer rise or fall over time is often more useful than a single value.
Why “non-reactive” does not always mean clear
Antibodies and antigens take time to build up. If you test too soon after a possible exposure, an infection can be real yet still invisible to the test. This is the single most common reason serology results are misread, and it is the focus of the next section.
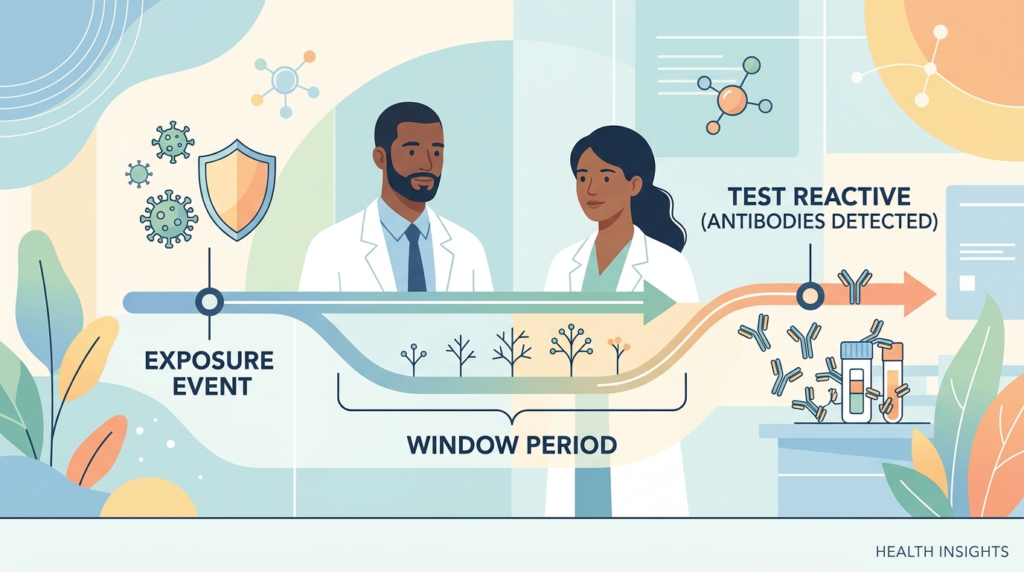
The window period: why timing changes your result
The window period is the gap between a possible exposure and the point when a test can reliably detect the infection. During this time a serology test can read non-reactive even though the infection is present, because your body has not yet made enough antibodies — a process called seroconversion.
Window periods differ by infection and by test:
- HIV laboratory antigen/antibody tests usually detect infection within about 18 to 45 days, while antibody-only and self-tests can take up to around 90 days.
- Many other STIs can take up to about seven weeks to show up. If you have no symptoms, waiting that long before testing lowers the chance of a falsely reassuring result.
If you tested early, your clinician may suggest repeating the test later, or using a different early test — such as a nucleic acid test (NAT) for HIV — when a recent exposure is a concern. In short, a non-reactive result is most trustworthy once the window period for that infection has passed.
When a serology result needs follow-up
A reactive or borderline result is a prompt for the next, more specific step — not a verdict. Depending on the infection, follow-up can include:
- A confirmatory test. For HIV, a different test confirms a reactive screen before any diagnosis is made.
- A panel of related markers. Hepatitis B, for example, is read as a small set of results together — surface antigen (HBsAg), surface antibody (anti-HBs), and core antibody (anti-HBc) — which together suggest current infection, past infection, or protection from vaccination. Because hepatitis can affect the liver, your clinician may also order liver function tests such as ALT and AST.
- A swab or PCR test. For herpes, an active sore is usually tested directly by PCR; blood (serology) HSV testing has limits and is not recommended as routine screening for everyone. If your mouth or throat is involved, see our guide to throat herpes.
Your results only make sense in the context of your symptoms, history, and any exposure. That is why the final interpretation is a conversation with a healthcare professional rather than a number read in isolation.
When to get a serology test or see a doctor
Testing is most useful when it matches your situation. Consider an STI and infectious disease panel — and a conversation with a clinician — if any of these apply:
- You have had a new partner, several partners, or a partner who has an STI.
- You have symptoms such as unusual discharge, pain when peeing, sores, or a rash.
- You are pregnant or planning a pregnancy, when screening is part of routine prenatal blood tests.
- You shared injection equipment, or you simply want a routine check as part of looking after your sexual health.
- A previous test fell inside the window period and needs repeating.
Seek prompt medical advice rather than waiting for a routine result if you have severe symptoms — for example a high fever, a spreading rash, severe pain, or feeling very unwell. These need assessment in their own right. It is also worth remembering that having had an infection once does not make you immune to getting it again.
Common infections a serology test can check
Several infections on a typical panel are picked up by serology, and a few common questions come up about them.
- HIV is screened with a combined antigen/antibody blood test and is highly manageable when found early.
- Syphilis is detected by a blood test with a confirming titer and is curable with antibiotics.
- Hepatitis B and hepatitis C are detected by blood tests. Both can be passed on through sex as well as through blood, which is why they appear on many STI panels, and both can affect the liver.
- Herpes (HSV) is usually diagnosed from a sore, with blood antibody testing reserved for specific situations rather than used for everyone.
Glossary
- Antibody: a protein the immune system makes to recognize a specific germ; finding one usually means past or present exposure.
- Antigen: a part of a germ itself; detecting an antigen points more directly to a current infection.
- HSV (herpes simplex virus): the virus that causes oral and genital herpes.
- IgG: an antibody type that appears later and often persists, marking past or resolved infection or long-term protection.
- IgM: an antibody type that usually appears first, suggesting a more recent infection.
- NAAT (nucleic acid amplification test): a test that finds a germ’s genetic material in urine or a swab, used for chlamydia, gonorrhea, and trichomoniasis.
- Reactive and non-reactive: the wording serology uses for “evidence found” (reactive) and “no evidence found” (non-reactive).
- Seroconversion: the point at which the body has made enough antibodies for a test to detect them.
- Serology: the branch of testing that examines blood for antibodies and antigens.
- Titer: a number, such as 1:8, showing how diluted the blood can be while still reacting; higher means more antibody.
Frequently asked questions
What is the difference between an STI and an STD?
The two terms describe the same group of infections, and many clinics now prefer “STI.” An STI (sexually transmitted infection) means a germ is present, often with no symptoms at all. STD (sexually transmitted disease) traditionally refers to an infection that has gone on to cause noticeable symptoms or complications. The tests are the same either way; the shift in wording reflects that most infections cause no symptoms, so “infection” is the more accurate term.
How long do STI test results take?
It depends on the test and the laboratory. Many results are ready within a few working days, and some rapid tests are quicker. Blood-based serology and tests sent to a central lab can take a little longer. If you tested at home, add the time it takes for your sample to reach the laboratory. Our guide to how long blood test results take covers typical turnaround times and when to follow up if results are late.
How long after a possible exposure should I wait to get tested?
This is the window period, and it varies by infection. Many STIs can take up to about seven weeks to show up, so if you have no symptoms it is often best to wait that long before testing. HIV laboratory tests usually detect infection within about 18 to 45 days. If you tested very early, your clinician may recommend repeating the test later, or an earlier test such as a NAT when a recent exposure is a concern.
Can you get an STI without having sex?
Yes. Some infections can spread through close skin-to-skin contact, such as herpes and HPV, and others — including hepatitis B and hepatitis C — can pass through blood or, in some cases, from parent to baby. Using condoms lowers the risk of many STIs but does not remove it entirely. A serology test and the rest of an STI panel can check for these infections regardless of how exposure may have happened.
Are hepatitis B and hepatitis C considered STIs?
They can be. Both are blood-borne viruses that can also be passed on through sexual contact, which is why they are commonly included on STI panels and detected by a serology test. Because both can affect the liver, a clinician may pair the result with liver markers such as ALT and AST. A reactive hepatitis result is read alongside other markers before any conclusion is drawn.
Should I get tested if I have no symptoms?
Often, yes. Many STIs cause no symptoms, which means you can carry an infection without knowing and pass it on. The only reliable way to know your status is to get tested. Routine screening is recommended for people who are sexually active, especially with new or multiple partners, even when they feel completely well. Testing without symptoms is normal and sensible, not a sign that anything is wrong.
Sources
- Antibody Serology Tests — MedlinePlus, U.S. National Library of Medicine
- Getting Tested for STIs — Centers for Disease Control and Prevention (CDC)
- Sexually transmitted infections (STIs) — NHS
Further reading
- How to read your blood test results
- How long do blood test results take?
- Blood tests during pregnancy: what is checked
- Liver function tests: how to read your results
- CBC vs CMP: understanding the tests
Understand your lab results with AI DiagMe
A serology test can raise as many questions as it answers, especially when a report lists terms like reactive, non-reactive, or a titer. AI DiagMe turns those numbers into clear, plain-language explanations for tests such as an HIV antigen/antibody screen, a syphilis test, or hepatitis B and C blood tests. It is built to help you understand what your results mean and what to ask next — not to diagnose you, and not as a replacement for your doctor. Upload your panel and see your results explained in minutes.
➡️ Get your results interpreted in minutes
{kind=link}