


















Blood tests during pregnancy are a routine part of prenatal care, and most people have several of them between their first visit and delivery. They are used to check your own health, confirm details like your blood type, screen for infections, and look at how your baby is developing. Seeing a long list of tests — or an unfamiliar value on a report — can feel confusing, especially when the terms are technical.
This guide explains, in plain language, which blood tests during pregnancy are usually done in each trimester, what each one checks, and how to make sense of common results. You will also find a timeline of when tests happen, a simple table of frequent markers, and clear signs of when to talk to your doctor. The goal is to help you walk into each appointment informed rather than anxious.
Why you have blood tests during pregnancy
Pregnancy changes how your body works, and some conditions that affect you or your baby cause no symptoms at all. Blood tests are a safe, low-risk way to spot these early, when they are easiest to manage.
Most prenatal blood tests fall into one of two groups. Screening tests estimate the chance that you or your baby has a certain condition. They do not give a yes-or-no answer. Diagnostic tests are used to confirm whether a condition is actually present, often after a screening test suggests a higher risk.
This difference matters. An abnormal screening result does not mean something is wrong — it means more information may be needed. It is also your choice whether to have prenatal tests. Some are recommended for nearly everyone because they catch treatable problems; others, especially genetic screening, are optional and personal.
Your very first blood draw usually happens once a home or clinic test has confirmed a pregnancy. If you want to understand how that early step works, see our pregnancy test guide.
First-trimester blood tests: what’s checked
The first trimester (roughly weeks 1 to 13) is when you have the most blood work. At your first prenatal visit, your provider draws blood for a group of tests often called the prenatal panel.
Blood type, Rh factor, and antibody screen
One of the first things checked is your blood type — A, B, AB, or O — along with your Rh factor, the “positive” or “negative” part of your type.
This matters because if you are Rh-negative and your baby is Rh-positive, your body could make antibodies against the baby’s red blood cells. An antibody screen checks for this. People who are Rh-negative are usually offered a medicine called Rh immunoglobulin (anti-D) around week 28 and again after birth if needed, to prevent problems in this or a future pregnancy.
Complete blood count (CBC)
A complete blood count (CBC) measures the different cells in your blood. Your provider looks at three main things: red blood cells, which can reveal anemia; white blood cells, which are part of your immune system; and platelets, which help your blood clot.
Pregnancy naturally increases the amount of fluid in your blood, which can make your hemoglobin and hematocrit look lower than usual. This dilution is normal, but true iron-deficiency anemia is also common in pregnancy. If your levels are low, your provider may check your iron stores (ferritin) and suggest iron-rich foods or a supplement.
Infection and immunity screening
Early blood tests also check for infections that could affect your baby if untreated. These typically include hepatitis B, hepatitis C, HIV, and syphilis. Your blood is also checked to see whether you are immune to rubella (German measles) and chickenpox. Some practices add a thyroid (TSH) check or vitamin levels depending on your history.
Finding an infection early is helpful, not alarming: in most cases, treatment or extra monitoring can greatly lower any risk to your baby.
Early genetic screening (combined test and NIPT)
If you choose it, genetic screening can start in the first trimester. Combined first-trimester screening pairs a blood test (measuring two pregnancy-related substances) with an ultrasound, usually around weeks 11 to 13. The ultrasound measures the small pocket of fluid at the back of the baby’s neck, while the blood test reads levels that shift in early pregnancy. When first- and second-trimester results are looked at together, the screening picks up more cases than either test on its own.
A newer option is cell-free DNA screening, also called noninvasive prenatal testing (NIPT). It looks at small fragments of the baby’s DNA that circulate in your blood and can be done from about the 10th week. It screens for certain chromosome conditions and can often reveal the baby’s sex. According to MedlinePlus, this test has almost no risk and a high rate of accuracy, but it remains a screening test, not a diagnosis.
Second- and third-trimester blood tests
After the busy first trimester, blood work becomes more targeted. The second trimester runs from about week 14 to week 27, and the third from around week 28 to birth.
The quad screen (AFP and more)
The quad screen is a second-trimester blood test, usually done between weeks 15 and 22. It measures four substances in your blood, including alpha-fetoprotein (AFP), a protein made by the baby’s liver.
The quad screen estimates the chance of Down syndrome, trisomy 18, and neural tube defects such as spina bifida. A higher-than-expected AFP level can point to a neural tube defect, but it can also simply mean twins or a different due date than expected. Because folate plays a key role in early spinal development, your provider may discuss your folate (vitamin B9) intake as well.
Glucose screening for gestational diabetes
Between about weeks 24 and 28, nearly everyone is offered a blood sugar (glucose) screening for gestational diabetes — a form of diabetes that can appear in pregnancy and usually goes away after birth. If you have risk factors, such as a higher body weight, a family history of diabetes, or gestational diabetes in a past pregnancy, your provider may screen you earlier and then repeat the test at the usual time.
For the screening, you drink a sweet liquid and have your blood drawn about an hour later. If that result is high, a longer glucose tolerance test confirms the diagnosis. Some providers also use HbA1c, which reflects your average blood sugar over recent months. Managed well, gestational diabetes most often leads to a healthy pregnancy.
Repeat tests later in pregnancy
Some first-trimester tests are repeated later. A CBC is often rechecked in the late second or third trimester to make sure anemia has not developed. If you are Rh-negative, your antibody screen may be repeated before you receive Rh immunoglobulin. A provider may also recheck a marker that was borderline earlier, so a second draw does not automatically mean something is wrong.
One common late test is not a blood test: the group B strep (GBS) check, done around weeks 36 to 37, uses a swab rather than a blood draw.
Genetic screening, explained: what these tests can and can’t tell you
Genetic blood tests cause some of the most common questions in pregnancy, partly because their names sound similar. Here is the key idea: these are screening tests. They tell you about probability, not certainty.
NIPT and the quad screen can flag a higher chance of conditions like Down syndrome (trisomy 21), trisomy 18, trisomy 13, and neural tube defects. They cannot, on their own, confirm that a baby has — or does not have — one of these conditions. A “screen positive” result usually leads to a conversation with your provider or a genetic counselor and, if you choose, a diagnostic test.
Diagnostic tests are different. Chorionic villus sampling (CVS), done around weeks 10 to 13, and amniocentesis, usually after week 15, take a small sample from the placenta or the fluid around the baby. They give a definitive answer but carry a small risk, so they are offered, not routine.
It is worth knowing what these tests do not do. They are not designed to screen for every condition, and no prenatal blood test can predict things like autism. A genetic counselor can help you decide which tests, if any, fit your situation.
Understanding common results on your prenatal blood test report
Lab reports list each marker with your value and a reference range. In pregnancy, some “normal” ranges shift, which is why your provider interprets results in context rather than by the numbers alone. The table below summarizes markers you are most likely to see.
| Marker | What it measures | Why it matters in pregnancy |
|---|---|---|
| Hemoglobin / hematocrit | Oxygen-carrying red blood cells | Screens for anemia; often dips slightly as blood volume rises |
| Platelets | Cells that help blood clot | A drop can occasionally signal a problem needing monitoring |
| White blood cells | Immune-system cells | Tend to rise in pregnancy; very high levels may suggest infection |
| Blood type and Rh | A/B/AB/O group and Rh factor | Guides whether you need Rh immunoglobulin |
| Ferritin | Stored iron | Low ferritin points to iron deficiency, common in pregnancy |
| Glucose | Blood sugar | Screens for gestational diabetes |
| AFP | Protein from the baby’s liver | Part of the quad screen for certain birth differences |
If a single value sits just outside its range, it is rarely a cause for worry on its own. Trends over time and your overall picture matter far more than one number.
How many blood tests during pregnancy will you have, and when?
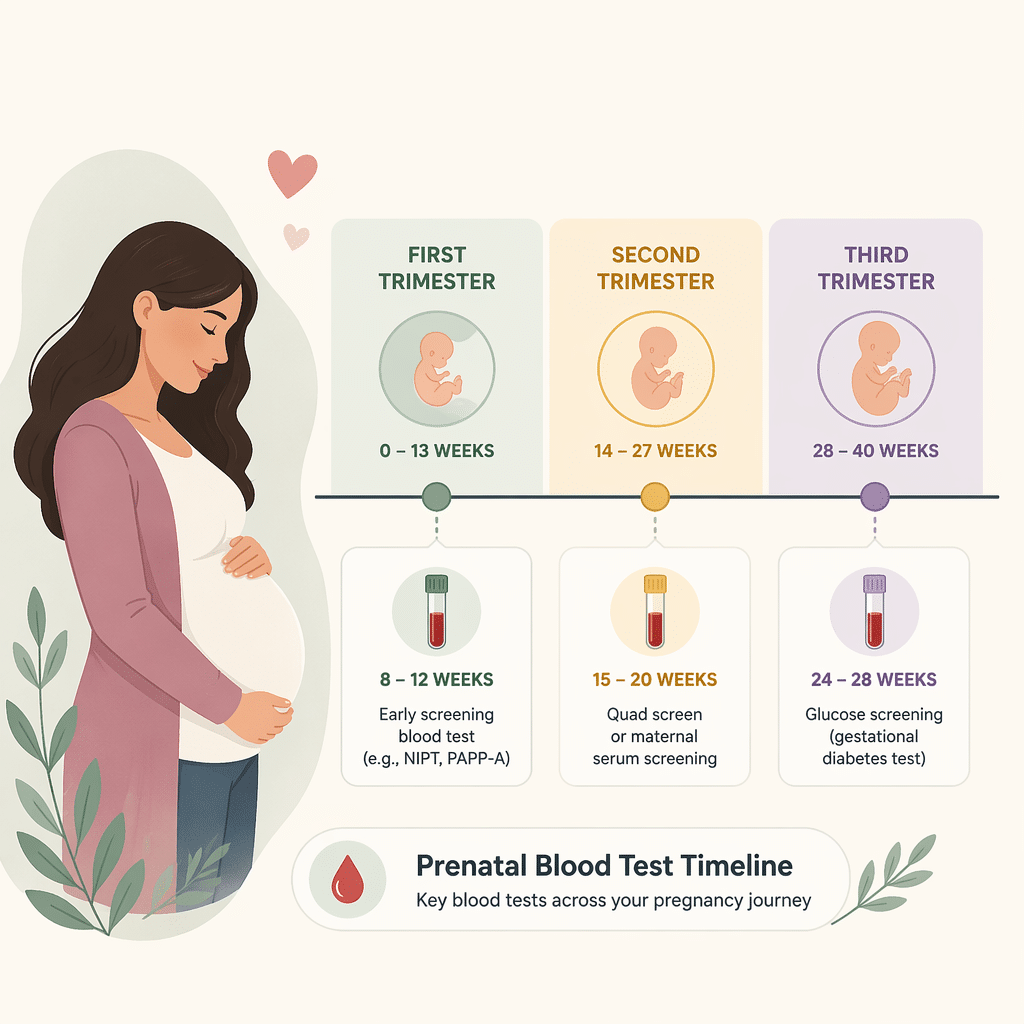
There is no single fixed number, but most low-risk pregnancies follow a similar rhythm. The timeline below shows when the main blood tests during pregnancy usually happen.
| Stage | Approximate timing | Typical blood tests |
|---|---|---|
| First visit | First trimester (weeks 4–12) | Blood type and Rh, antibody screen, CBC, infection and immunity screening |
| Early genetic screening | Weeks 10–13 | Cell-free DNA (NIPT) or combined first-trimester screening |
| Second-trimester screening | Weeks 15–22 | Quad screen (including AFP) |
| Glucose screening | Weeks 24–28 | One-hour glucose screening (then tolerance test if needed) |
| Late pregnancy | Weeks 28 onward | Repeat CBC, repeat antibody screen if Rh-negative |
If you have a health condition, a multiple pregnancy, or a higher-risk pregnancy, your provider may add tests or repeat them more often. That is normal and tailored to keep you and your baby well.
When to talk to your doctor about your results
Your care team will contact you about results that need attention, and you do not have to interpret reports alone. Still, it helps to know when to reach out.
Contact your provider promptly if you notice any of the following:
- A result labeled “abnormal,” “positive,” or “high risk” that no one has explained to you yet
- Symptoms of anemia, such as unusual tiredness, dizziness, or shortness of breath
- Signs of high blood sugar, such as excessive thirst or frequent urination beyond what is usual in pregnancy
- A fever or symptoms of infection after an abnormal screening result
- Any result you simply do not understand and want clarified before your next visit
Seek urgent care for warning signs such as heavy vaginal bleeding, severe or persistent abdominal pain, a bad headache with vision changes, or noticeably reduced baby movements later in pregnancy. These are not specific to blood tests, but they always deserve prompt attention.
Glossary
- AFP (alpha-fetoprotein): A protein made by the baby’s liver and measured in the quad screen; unusual levels may prompt further testing.
- Cell-free DNA (NIPT): A blood test that examines fragments of the baby’s DNA in the mother’s blood to screen for certain chromosome conditions.
- Complete blood count (CBC): A test that counts red cells, white cells, and platelets, used to check for anemia, infection, and clotting issues.
- Ferritin: A protein that stores iron; a low level usually indicates iron deficiency.
- Gestational diabetes: A form of high blood sugar that develops during pregnancy and most often resolves after birth.
- Hematocrit: The share of your blood made up of red blood cells, used to assess anemia.
- Quad screen: A second-trimester blood test measuring four substances to estimate the chance of certain conditions.
- Rh factor: A protein on red blood cells that makes your blood type “positive” or “negative.”
- Trimester: A roughly three-month stage of pregnancy; there are three in total.
Frequently asked questions
Is there a blood test for autism during pregnancy?
No. There is currently no blood test that can diagnose autism before birth. Prenatal genetic screening, including cell-free DNA testing (NIPT), looks at the chance of certain chromosome conditions, such as Down syndrome — it does not screen for autism. Autism is usually identified in early childhood through developmental check-ups, not pregnancy blood work. If you have a family history of autism or developmental conditions and want to understand your options, a genetic counselor can talk through what prenatal tests can and cannot tell you.
Can a blood test tell my baby’s sex?
Often, yes. Cell-free DNA screening (NIPT) analyzes fragments of the baby’s DNA in your blood and can frequently identify the baby’s sex from around the 10th week of pregnancy, alongside screening for certain chromosome conditions. Accuracy is high but not absolute, and results can occasionally be unclear. An ultrasound later in pregnancy is another common way to check. Keep in mind that NIPT is mainly a screening test for the baby’s health; sex information is an added detail, not its main purpose.
Can I refuse blood tests during pregnancy?
Yes. Prenatal tests are offered to you, and it is your choice whether to have them. Many tests — such as blood type, infection screening, and glucose screening — are recommended for nearly everyone because they catch problems that are treatable during pregnancy. Others, especially genetic screening, are optional and personal. If you are unsure, ask your provider what a specific test checks for, what the results could mean, and what happens if you decline. Understanding the purpose can help you make a decision you feel comfortable with.
Do I need to fast before pregnancy blood tests?
Usually not. Most routine prenatal blood tests, including your blood type, complete blood count, and infection screening, do not require fasting. The main exception involves blood sugar tests. The one-hour glucose screening does not normally need fasting, but the longer glucose tolerance test, used when the first result is high, does require you to fast beforehand. Your clinic will tell you in advance if a particular test needs an empty stomach, so follow their specific instructions.
Can a blood test confirm paternity during pregnancy?
Yes. A noninvasive prenatal paternity test compares cell-free DNA from the baby, found in the mother’s blood, with a DNA sample from the possible father. It can often be done from around the 7th to 9th week of pregnancy and carries no risk to the baby, unlike older methods that sampled fluid or tissue from the womb. These tests are usually arranged through specialized laboratories rather than routine prenatal care. For legally recognized results, choose an accredited lab and ask how samples are collected and verified.
Can a blood test detect pregnancy during implantation bleeding?
Sometimes, but timing matters. A blood test measures hCG, a hormone your body makes once a fertilized egg implants in the uterus. Implantation bleeding, if it happens, occurs very early — often before hCG has risen enough to be detected. A blood test is more sensitive than a urine test and can pick up pregnancy a few days earlier, but testing too soon can still give a negative result. Waiting until around the time of your missed period gives a more reliable answer.
Sources
- Mayo Clinic — Prenatal testing: Is it right for me?
- MedlinePlus (National Library of Medicine, NIH) — Prenatal Testing
- Yale New Haven Health — Prenatal Screenings in the First, Second and Third Trimester
Further reading
- CBC vs CMP: Understanding the Tests
- Understanding the Rh System: Causes & Risks
- Fasting Blood Glucose: Your Complete Guide to Interpretation
- Alpha-fetoprotein (AFP): Understanding Your Blood Test Results
- Pregnancy Test Guide: Accuracy and Interpretation
Understand your lab results with AI DiagMe
Your prenatal panel can include a lot at once — a complete blood count (CBC), your blood type and Rh factor, infection screening, iron stores (ferritin), and a blood sugar (glucose) check for gestational diabetes. If your report leaves you with questions before your next appointment, AI DiagMe can help you understand what each value means in clear, everyday language. Reviewed by a panel of doctors and with your data hosted securely, it is built to help you make sense of your results — not to diagnose you or replace your care team. Bring your questions to your provider, and use AI DiagMe to feel prepared.
➡️ Get your results interpreted in minutes

{kind=link}