

















Liver function tests are a group of blood markers that show how your liver is working and whether its cells are under strain. If you are holding a report covered in abbreviations like ALT, AST, ALP, GGT and bilirubin, this guide walks you through what each number means, what counts as a normal range, and why doctors look at the pattern of results rather than any single value. You will also learn what high results can point to, how high is “high,” when normal numbers can still hide a problem, and which warning signs should prompt a call to your doctor. The aim is to help you read your own liver panel with confidence, not to replace the conversation with your healthcare provider.
What liver function tests actually measure
The name is a little misleading. Most of what a standard liver panel measures are not measures of “function” at all, but signs of liver cell injury or bile flow problems. Only a few values truly reflect how well the liver is doing its day-to-day jobs.
Doctors order this panel for several reasons: as part of a routine check-up, to investigate symptoms such as tiredness, jaundice or abdominal pain, to screen people with risk factors like diabetes or heavy alcohol use, and to monitor a known condition or a medicine that can affect the liver. Knowing why yours was ordered helps you read the result in the right context.
It helps to split the panel into two groups. The first group is enzymes that leak into the blood when liver cells are damaged or irritated. The second group reflects the liver’s actual work: making proteins and clearing waste.
The enzymes that signal injury are alanine aminotransferase (ALT) and aspartate aminotransferase (AST), which sit inside liver cells, plus alkaline phosphatase (ALP) and gamma-glutamyl transferase (GGT), which rise mainly when bile flow is blocked.
The markers that reflect real function are albumin and total protein (proteins the liver builds) and bilirubin (a yellow waste pigment the liver clears). Clotting tests such as PT/INR also belong here, because the liver makes most clotting factors.
Many of these tests appear inside a wider panel called the comprehensive metabolic panel (CMP), so you may see them grouped with kidney and sugar results on the same report.
Here is what each common item on a liver panel reflects:
| Test | What it mainly reflects | In plain words |
|---|---|---|
| ALT | Liver cell injury | A fairly specific signal that liver cells are leaking |
| AST | Liver and muscle cell injury | Less liver-specific; can also rise from muscle or heart |
| ALP | Bile ducts and bone | Rises with blocked bile flow, and sometimes with bone activity |
| GGT | Bile ducts | Helps confirm a high ALP is from the liver; rises with alcohol and some medicines |
| Total bilirubin | Bile pigment processing | A high level can cause yellow skin or eyes (jaundice) |
| Direct (conjugated) bilirubin | Bile flow and excretion | Helps separate a bile-flow problem from red blood cell breakdown |
| Albumin | Liver protein production | A low level can suggest long-standing liver disease |
| Total protein | Overall protein, including liver-made proteins | Read alongside albumin for context |
Normal ranges for a liver panel
Before you panic about a number, find the range printed next to it on your own report. Reference ranges differ between laboratories, between men and women, and across age groups, so a value that is “high” at one lab may be normal at another.
The values below are commonly used adult ranges. Treat them as a guide only, not as a verdict on your health.
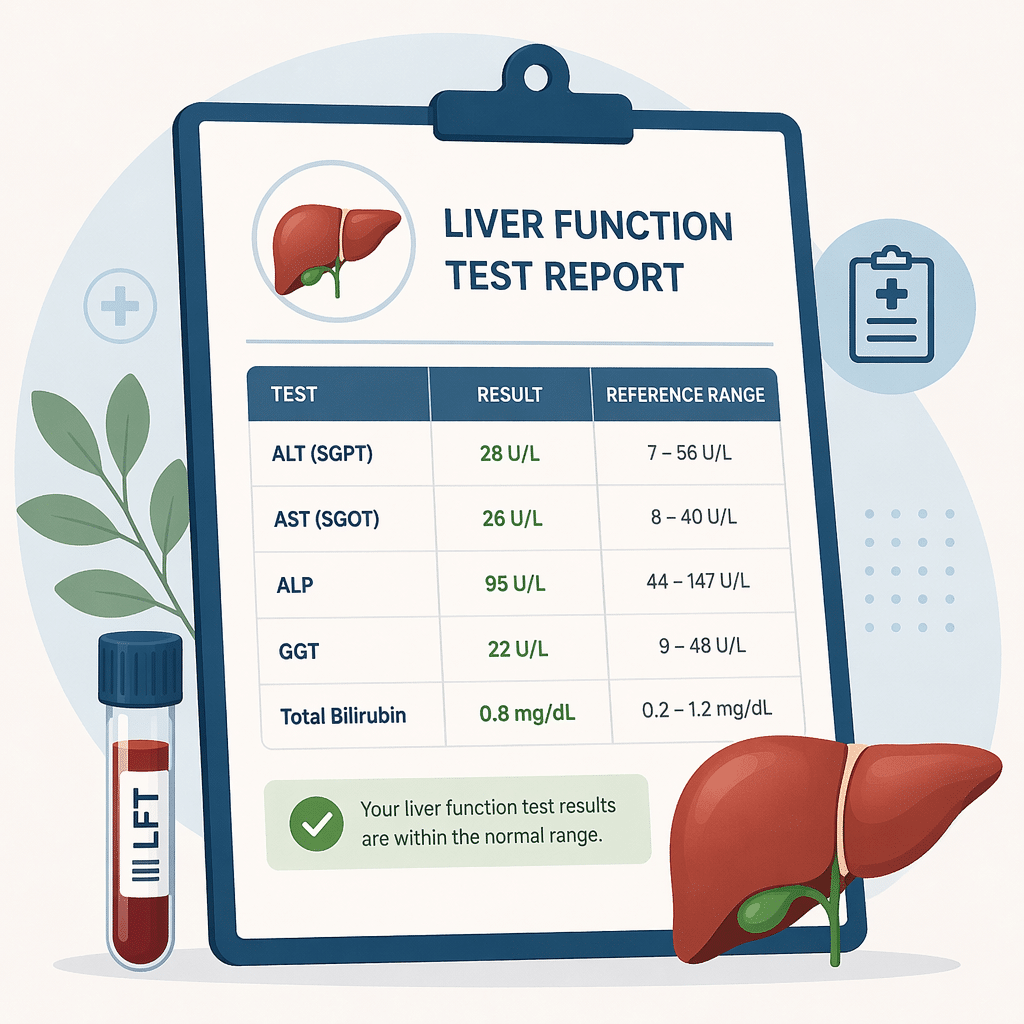
| Test | Typical adult range* | Common unit |
|---|---|---|
| ALT | 7–55 | U/L |
| AST | 8–48 | U/L |
| ALP | 40–130 | U/L |
| GGT | 8–61 | U/L |
| Total bilirubin | 0.1–1.2 | mg/dL |
| Direct bilirubin | 0.0–0.3 | mg/dL |
| Albumin | 3.5–5.0 | g/dL |
| Total protein | 6.0–8.3 | g/dL |
*Ranges are approximate and vary by laboratory, sex and age. Always read your result against the range printed on your own report.
One nuance worth knowing: some specialists argue the “true” healthy upper limit for ALT is lower than many labs use, because standard ranges were partly set using people who already had mild, undetected liver issues. This is why a result at the top of the normal band, repeated over time, can still be worth a conversation.
How to read your liver function tests as a pattern
This is the single most useful idea in the whole guide. Doctors rarely read one marker in isolation. Instead, they look at which group of markers is raised, and by how much, to sort the result into a recognisable pattern.
There are three broad patterns. Recognising yours tells you far more than any single number.
| Pattern | Markers that rise most | Common causes |
|---|---|---|
| Hepatocellular (cell injury) | ALT and AST | Fatty liver, viral hepatitis, medicines, alcohol |
| Cholestatic (blocked bile flow) | ALP and GGT, often with bilirubin | Gallstones, a blocked bile duct, certain medicines |
| Mixed | Both groups together | Some drug reactions, more advanced liver disease |
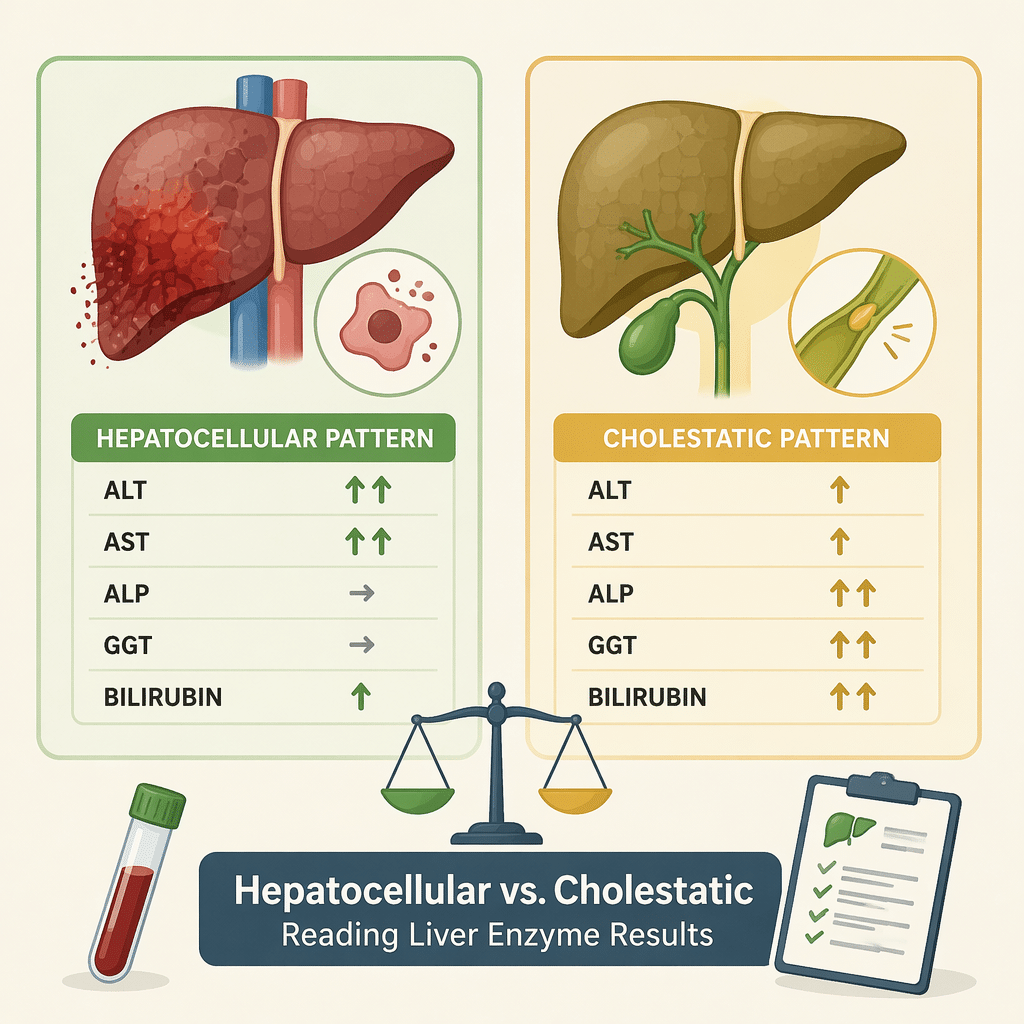
A practical tip: if ALP is high, GGT helps tell you where it is coming from. When both ALP and GGT are raised, the source is usually the liver or bile ducts. When ALP is high but GGT is normal, the cause is more likely bone, such as normal growth in children.
The AST/ALT ratio
Comparing AST to ALT gives an extra clue. In most common causes, including fatty liver, ALT is higher than AST, so the ratio sits below 1. When AST is clearly higher than ALT, with a ratio above 2, alcohol-related liver disease becomes more likely. Ratios are hints, not proof, and your doctor weighs them against your history, medicines and other tests.
As a quick example, imagine a report with a mildly high ALT, a slightly high AST, normal ALP and normal bilirubin. That is a hepatocellular pattern, mild in degree, with a ratio below 1, a picture that very often reflects fatty liver. By contrast, a high ALP and GGT with a rising bilirubin, but only modest ALT and AST, points instead toward a bile-flow problem and a different set of next steps.
What high liver function tests can mean
A high result is common and often has a simple, reversible cause. The most frequent reason worldwide is metabolic dysfunction-associated steatotic liver disease (MASLD), the condition that used to be called non-alcoholic fatty liver disease. It is strongly linked to weight, blood sugar and cholesterol, and it often causes mild enzyme rises with no symptoms at all.
Other common causes include regular or heavy alcohol use, certain medicines and supplements, viral infections such as hepatitis B and hepatitis C, and iron overload, also called hemochromatosis.
Medicines and supplements deserve their own mention, because they are an easily missed cause. Everyday painkillers such as acetaminophen (paracetamol), some cholesterol-lowering statins, certain antibiotics and a number of “natural” products, including high-dose green tea extract and some bodybuilding supplements, can all raise liver enzymes. This is why your doctor will ask for a complete list, prescription and over-the-counter alike.
Finally, remember that AST is not liver-specific. Because it also sits in muscle and heart, a recent hard workout, a muscle injury or a heart problem can lift AST, and sometimes ALT, without the liver being involved at all.
How high is high?
The degree of elevation matters as much as the fact that a marker is raised. A value just over the limit is read very differently from one that is many times higher.
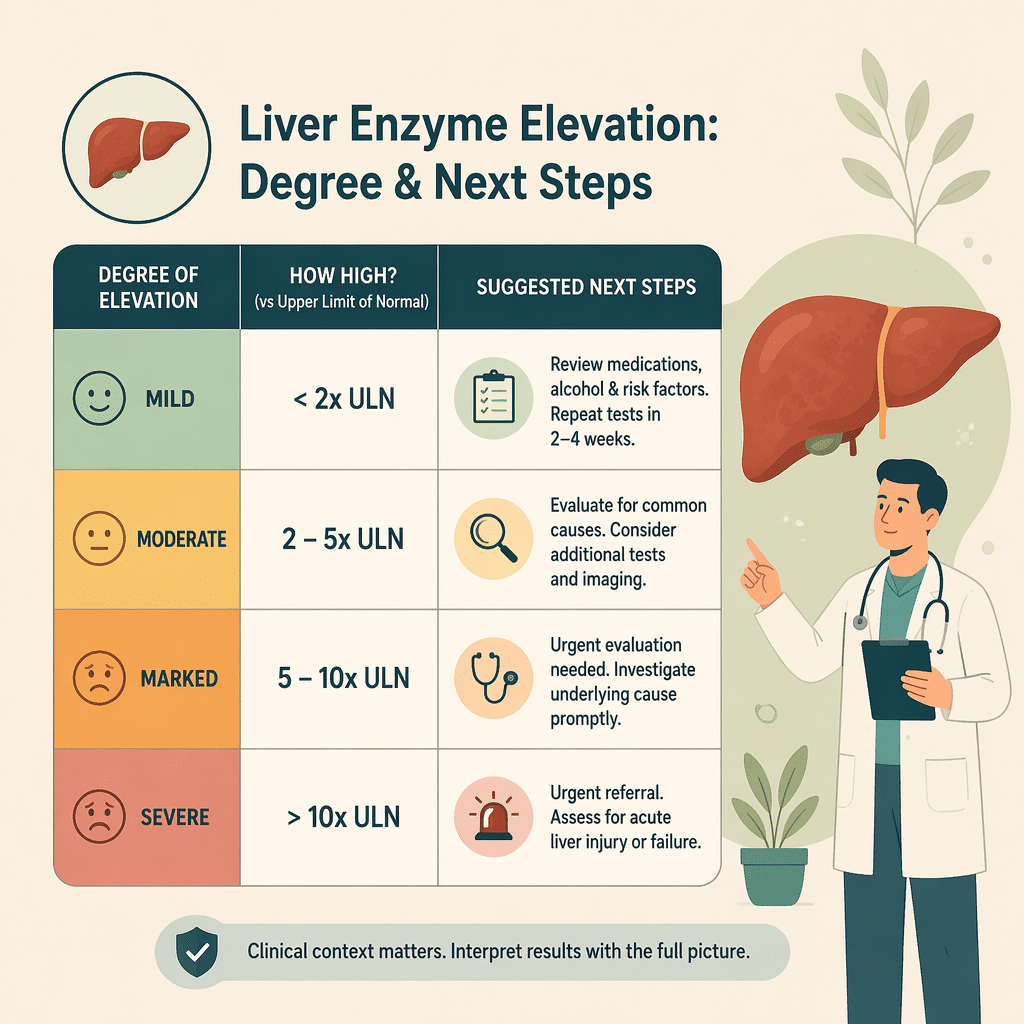
| Degree | Roughly how high | What it can suggest | Usual next step |
|---|---|---|---|
| Mild | Under 3× the upper limit | Fatty liver, recent alcohol, some medicines, recent infection | Often a repeat test in a few weeks |
| Moderate | 3–10× the upper limit | Active inflammation, hepatitis, a drug effect | Further blood tests, sometimes imaging |
| Marked | Over 10× (ALT or AST often above 1,000 U/L) | Acute liver injury, such as an acetaminophen (paracetamol) overdose or acute viral hepatitis | Prompt medical assessment |
Mild rises frequently settle on their own, which is why repeat testing is so common before anyone reaches for a diagnosis. If a raised ALT is linked to lifestyle, your doctor may suggest changes and recheck; you can read more about the factors behind a high ALT and what tends to help.
A step-by-step way to read your liver panel
Putting it all together, you can work through your report in a logical order rather than reacting to the first scary number. This is roughly the same sequence a clinician follows.
- Find your own ranges. Read each value against the reference range printed on your report, not a range from the internet.
- Mark what is out of range. Note which markers are high or low, and ignore the ones that are normal for now.
- Spot the pattern. Are ALT and AST leading (hepatocellular), or ALP and GGT (cholestatic), or both (mixed)?
- Check the degree. Is the rise mild, moderate or marked? A value just over the limit is very different from one many times higher.
- Look at the function markers. Glance at albumin, bilirubin and any clotting result, which say more about how the liver is coping.
- Add your context. Factor in alcohol, new medicines or supplements, recent exercise and any symptoms.
- Plan the follow-up with your doctor. Decide together whether to repeat the test, add others, or arrange a scan.
Working through these steps turns a confusing printout into a short, answerable list of questions for your appointment.
When normal results don’t mean a healthy liver
It feels reassuring to see every value inside the range, and usually it is good news. But normal liver function tests do not completely rule out liver disease, for three reasons.
First, the liver has a large reserve, so enzymes can be normal even when scarring is building quietly. Advanced scarring, or cirrhosis, can sometimes show near-normal enzymes because there are fewer healthy cells left to leak them.
Second, fatty liver disease is often silent and can come and go on blood tests. A single normal panel is a snapshot, not a guarantee.
Third, the enzymes that catch injury are not the same as the markers that show how badly function is affected. When doctors want to judge severity, they look more closely at albumin, bilirubin and clotting, often through a PT/INR (prothrombin time) test. A falling albumin, a rising bilirubin or a longer clotting time can matter more than a modest enzyme bump.
When to see a doctor about your liver panel
Most abnormal liver function tests are not emergencies, and your doctor will guide the timing. Still, some signs deserve prompt attention rather than waiting for a routine appointment.
Contact a doctor without delay if abnormal results come with any of the following:
- Yellowing of the skin or the whites of the eyes (jaundice)
- Dark urine together with pale, putty-coloured stools
- Severe or persistent pain in the upper right side of the abdomen
- Easy bruising or bleeding, or vomiting blood
- Swelling of the abdomen or legs
- Confusion, drowsiness or unusual sleepiness
It is also sensible to book a review, less urgently, if a value stays raised on a repeat test, if it is climbing over time, or if more than one marker is abnormal at once. When you go, bring a full list of your medicines, supplements and recent alcohol intake, since all three commonly affect results. Your doctor may simply repeat the panel, add tests such as viral or iron studies, or arrange an ultrasound scan to see the liver directly.
Glossary
- Albumin: The main protein made by the liver. A low level can point to long-standing liver or kidney problems, or poor nutrition.
- Alkaline phosphatase (ALP): An enzyme that rises mainly when bile flow is blocked, and sometimes with bone activity.
- Alanine aminotransferase (ALT): A fairly liver-specific enzyme that leaks into the blood when liver cells are damaged.
- Aspartate aminotransferase (AST): An enzyme found in the liver, muscle and heart, so it is less specific to the liver than ALT.
- Bilirubin: A yellow waste pigment from old red blood cells; a high level can cause jaundice.
- Cholestatic pattern: A result where ALP and GGT (and often bilirubin) are the markers most raised, suggesting a bile flow problem.
- Gamma-glutamyl transferase (GGT): A bile-duct enzyme that helps confirm whether a high ALP comes from the liver; it also rises with alcohol and some medicines.
- Hepatocellular pattern: A result where ALT and AST are the markers most raised, suggesting liver cell injury.
- Reference range: The set of values a laboratory considers normal for a given test, which can differ by lab, sex and age.
- Upper limit of normal (ULN): The top value of a reference range; “3× the ULN” simply means three times that top number.
Frequently asked questions
Do I need to fast before a liver function test?
For the liver markers themselves, fasting is usually not required, since ALT, AST, ALP and bilirubin are not greatly changed by a recent meal. However, liver tests are often ordered together with glucose and cholesterol as part of a wider panel, and those tests may need you to fast for several hours. Always follow the specific instructions on your test request, and if you are unsure, ask the clinic or laboratory before your appointment. Arriving fasted when it was not needed is harmless, but skipping a needed fast can delay results.
How long should I avoid alcohol before a liver function test?
There is no single official cut-off, but avoiding alcohol for at least 24 hours before the test is a reasonable rule, since a recent drinking session can temporarily raise GGT and other enzymes. If your doctor is checking whether alcohol is affecting your liver, they may ask you to abstain for longer, often a few weeks, and then repeat the test. A clear drop on the repeat sample is itself useful information. Be honest about your usual intake, because it helps your doctor interpret the numbers correctly.
What does a high bilirubin with normal enzymes mean?
A raised bilirubin alongside completely normal enzymes is often harmless. A common explanation is Gilbert’s syndrome, a very frequent inherited trait where bilirubin rises mildly during fasting, stress or illness and causes no harm. Other causes include faster-than-usual breakdown of red blood cells. Because the pattern can occasionally point to a bile or blood problem, your doctor may split the result into direct and indirect bilirubin and check a few related tests. If everything else is normal and you feel well, the finding is usually reassuring rather than worrying.
Can liver function tests be normal with cirrhosis?
Yes, and this surprises many people. In cirrhosis, much of the liver has been replaced by scar tissue, so there may be fewer healthy cells left to release enzymes, leaving ALT and AST near normal. This is why doctors do not rely on enzymes alone to rule out serious disease. They also look at albumin, bilirubin, platelet counts and clotting, and may use scans or specific scoring tools. If you have risk factors for liver scarring, normal enzymes should not stop you from discussing further assessment with your doctor.
Are high liver enzymes always serious?
No. Mild elevations are common and frequently have everyday, reversible causes such as fatty liver, recent alcohol, a viral illness, intense exercise or a new medicine. Many borderline results return to normal on their own within a few weeks. What matters is the size of the rise, whether it is persistent or climbing, whether several markers are affected together, and whether you have any symptoms. Your doctor reads the numbers in context rather than treating a single high value as an automatic cause for alarm.
How often should liver function tests be repeated?
It depends entirely on the reason for testing. A one-off mild abnormality is often rechecked once after a few weeks to see if it settles. If you have an ongoing condition such as fatty liver, hepatitis or a medicine that can affect the liver, your doctor may schedule regular monitoring, anywhere from every few months to once a year. There is no universal schedule, so follow the plan your healthcare provider sets based on your individual situation.
Sources
- Liver Function Tests — MedlinePlus (U.S. National Library of Medicine, NIH)
- Liver Function Tests: Types, Purpose & Results Interpretation — Cleveland Clinic
- Assessing liver function and interpreting liver blood tests — NHS Specialist Pharmacy Service
Further reading
- Alanine aminotransferase (ALT) levels explained
- AST (SGOT) blood test: meaning and results
- Gamma-glutamyl transferase (GGT): a complete guide
- Alkaline phosphatase (ALP) test explained
- CBC vs CMP: understanding the tests
Understand your lab results with AI DiagMe
Reading a liver panel means joining the dots between several markers at once, and that is hard to do alone with a printout full of abbreviations. AI DiagMe helps you make sense of results such as your liver enzymes (ALT and AST), your bile-flow markers (ALP and GGT), bilirubin and the proteins your liver makes, putting each value in plain language and in context. It is built to help you understand your numbers and prepare better questions, not to give a diagnosis or replace your doctor. If you have a recent report in hand, let AI DiagMe walk you through what it shows.
➡️ Get your results interpreted in minutes
{kind=link}