














Hereditary spherocytosis is an inherited blood disorder in which red blood cells lose their normal flexible disc shape and become small spheres that break down too early. This early breakdown, called hemolysis, leads to a long-lasting form of anemia, yellowing of the skin and eyes (jaundice), and an enlarged spleen. It is the most common inherited cause of hemolytic anemia in people of Northern European ancestry. In this article you will learn what hereditary spherocytosis is, what causes it, how doctors diagnose it through blood tests, how it is treated, and what recent research on new gene variants means for patients and families.
What is hereditary spherocytosis?
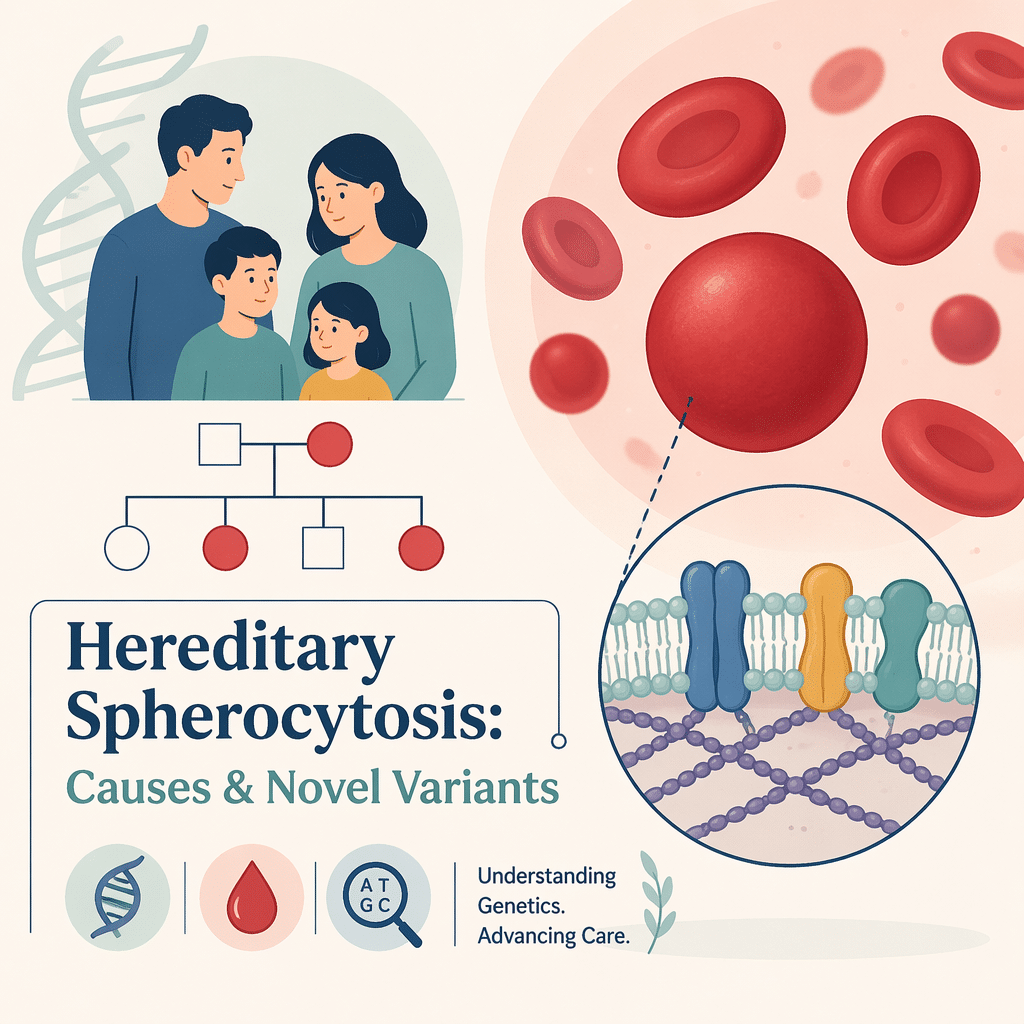
Hereditary spherocytosis is a condition of the red blood cell membrane, the flexible outer wall that lets each cell bend and squeeze through narrow blood vessels. In this disorder, the proteins that hold that membrane together are faulty, so the cell cannot keep its usual flattened, doughnut-like shape. Instead it becomes a rigid sphere known as a spherocyte.
These spheres are fragile and do not pass easily through the spleen, the organ that filters old or damaged blood cells. The spleen traps and destroys spherocytes faster than the bone marrow can replace them. The result is a shortage of red blood cells and a build-up of their breakdown products. Hereditary spherocytosis affects roughly 1 in 2,000 people of Northern European descent, and it can appear at any age, from newborns to adults with milder forms.
What causes hereditary spherocytosis?
Hereditary spherocytosis is caused by changes (variants) in genes that provide the instructions for red blood cell membrane proteins. At least five genes are involved: ANK1, SPTB, SPTA1, SLC4A1 and EPB42. Together they make proteins with names such as ankyrin, spectrin, band 3 and protein 4.2. When one of these proteins is missing or abnormal, the membrane loses stability and the cell collapses into a sphere. Variants in the ANK1 gene account for about half of all cases.
How it is inherited
In about three out of four families, hereditary spherocytosis is passed on in an autosomal dominant pattern, which means a single altered gene copy from one parent is enough to cause the condition. Less often it follows an autosomal recessive pattern, where a child inherits an altered copy from each parent. Some people are the first in their family to be affected because the change arose new in them. Because the inheritance pattern matters for relatives, testing often extends to parents, siblings and children.
Symptoms and how severe it can be
The features of hereditary spherocytosis come from two things: too few red blood cells, and the breakdown products those cells leave behind. Common signs include tiredness, paleness, shortness of breath and a fast heartbeat, which are the usual symptoms of anemia. Jaundice is frequent, especially in newborns, because a pigment called bilirubin builds up as red cells break down. Many people develop an enlarged spleen, and gallstones are common because excess bilirubin can form hard deposits in the gallbladder.
Hereditary spherocytosis varies widely from one person to the next. Doctors describe four broad forms based on severity, summarised below.
| Form | Approximate share of cases | What it usually looks like |
|---|---|---|
| Mild | 20–30% | Little or no anemia; sometimes found only in adulthood |
| Moderate | 60–70% | Anemia, jaundice and an enlarged spleen, often noticed in childhood; gallstones common |
| Moderate to severe | About 10% | All moderate features plus more pronounced anemia |
| Severe | 3–5% | Life-threatening anemia needing regular transfusions; marked spleen enlargement |
How hereditary spherocytosis is diagnosed
Diagnosis combines your personal and family history with a set of blood tests. Doctors first order a complete blood count to confirm anemia and to look for clues such as a high mean corpuscular hemoglobin concentration (MCHC), which is typical of this condition. A peripheral blood smear lets a specialist see spherocytes under the microscope, and a reticulocyte count shows whether the bone marrow is releasing extra young red cells to compensate.
To confirm that red cells are being destroyed, laboratories measure lactate dehydrogenase, check bilirubin, and test the blood protein haptoglobin. Specialised tests then support the diagnosis: the eosin-5-maleimide (EMA) binding test, the osmotic fragility test and the acidified glycerol lysis test all assess how easily red cells break. When results are unclear or a precise cause is needed, genetic testing identifies the exact variant.
| Test | What it checks |
|---|---|
| Complete blood count (CBC) | Whether anemia is present and whether the MCHC is high |
| Peripheral blood smear | Whether spherocytes are visible under the microscope |
| Reticulocyte count | Whether the marrow is making extra young red cells |
| Bilirubin, LDH and haptoglobin | Signs that red cells are breaking down (hemolysis) |
| EMA binding test | A flow-cytometry result strongly suggestive of the condition |
| Osmotic fragility or AGLT | Whether red cells burst more easily than normal |
| Genetic testing (NGS) | The exact gene variant responsible |
Treatment and management
There is no cure for hereditary spherocytosis, but the condition is very manageable and most people live full, healthy lives. Care focuses on supporting red blood cell production, preventing complications, and treating them promptly when they arise. Because the bone marrow works overtime to replace lost cells, it uses up extra folate; for this reason many people take daily folic acid supplements, particularly in moderate or severe disease.
People with more severe anemia may need blood transfusions, and newborns with marked jaundice may receive light therapy (phototherapy) to lower bilirubin. When red cell destruction is severe, surgeons may remove all or part of the spleen, an operation called splenectomy, which often reduces anemia because the spleen is where spherocytes are destroyed. Splenectomy is reserved mainly for moderate-to-severe disease because living without a spleen raises the long-term risk of serious infection; vaccination against pneumococcus, meningococcus and Haemophilus influenzae beforehand is essential.
Long-term follow-up also watches for gallstones and for the effects of frequent transfusions. Some people who receive regular transfusions develop iron overload, so doctors may order a complete iron studies panel and, when needed, treatment to remove excess iron.
When to see a doctor
Seek medical advice if you or your child have ongoing tiredness, paleness, yellowing of the eyes or skin, or upper-abdominal pain that could signal gallstones. A sudden drop in energy with worsening paleness can mean a temporary halt in red cell production, sometimes triggered by a viral infection, and should be checked quickly. Anyone with a family history of hereditary spherocytosis or unexplained chronic anemia should mention it, because it guides testing.
Latest scientific advances
Research over the past few years has made hereditary spherocytosis easier to confirm and to understand. Two themes stand out, and both are good news for patients.
First, diagnosis is becoming more precise. A 2025 overview of how the condition is identified describes how modern blood-cell analysers now flag subtle clues automatically, and how the EMA binding test and genetic sequencing increasingly work side by side (Polizzi et al., Int J Lab Hematol, 2025). What this means for you: a clearer answer from a simple blood sample, often without the slower, more cumbersome tests of the past.
Second, the catalogue of known gene variants keeps growing. Next-generation sequencing — a technique that reads the spelling of many genes at once — regularly uncovers changes that had never been described before; a 2024 report, for example, identified a brand-new variant in the SPTB gene (Wang et al., BMC Med Genomics, 2024). What this means for you: even when older tests are inconclusive, genetic testing can pinpoint the exact cause, confirm a diagnosis that runs in the family, and help doctors anticipate how mild or severe the condition is likely to be. These results are still being gathered in larger groups of patients, so the genotype-phenotype links are expected to sharpen further in the coming years.
Glossary
| Term | Definition |
|---|---|
| Spherocyte | A red blood cell that has become sphere-shaped instead of a flexible disc, making it fragile. |
| Hemolysis | The breakdown of red blood cells faster than the body can replace them. |
| Hemolytic anemia | A shortage of red blood cells caused by their early destruction. |
| Reticulocyte | A young red blood cell newly released from the bone marrow. |
| Splenomegaly | An enlarged spleen. |
| Splenectomy | Surgery to remove all or part of the spleen. |
| EMA binding test | A flow-cytometry blood test used to help confirm hereditary spherocytosis. |
| Osmotic fragility test | A test of how easily red blood cells burst in a dilute solution. |
| Bilirubin | A yellow pigment released when red cells break down; high levels cause jaundice. |
| MCHC | Mean corpuscular hemoglobin concentration, a CBC value often raised in this condition. |
Frequently asked questions
Is hereditary spherocytosis serious?
For most people it is not. The majority have mild or moderate disease and a normal life expectancy with simple monitoring. A small minority have severe anemia that needs regular transfusions or surgery. Even in these cases, effective treatments are available, and outcomes are generally good with proper follow-up.
Is hereditary spherocytosis a type of cancer?
No. It is a benign, inherited disorder of the red blood cell membrane. It is not a cancer and does not turn into one. The anemia it causes comes from red cells breaking down too quickly, not from any malignant growth in the blood or bone marrow.
Will my children inherit hereditary spherocytosis?
It depends on the inheritance pattern in your family. In the common autosomal dominant form, each child of an affected parent has roughly a 50% chance of inheriting the condition. In the rarer recessive form, both parents must pass on an altered gene. A genetic counsellor can explain the specific risk for your family and the testing options.
Does folic acid help hereditary spherocytosis?
Yes, it can be helpful. Because the bone marrow makes red blood cells faster than usual, it consumes more folate. Folic acid supplements replace what is used up and support healthy red cell production, which is why doctors often recommend them, especially in moderate or severe disease. Always follow your own doctor’s advice on dosing.
Is a splenectomy always needed?
No. Removing the spleen is reserved mainly for moderate-to-severe cases where anemia significantly affects daily life. Many people never need it. Because the spleen helps fight infection, the decision weighs the benefits against a lifelong higher infection risk, and vaccinations are given beforehand.
What is the life expectancy with hereditary spherocytosis?
Most people with hereditary spherocytosis have a normal life expectancy and quality of life. With routine check-ups, folate support when needed, and prompt treatment of complications such as gallstones, the long-term outlook is generally very good.
Sources
- MedlinePlus Genetics (NIH/NLM): Hereditary spherocytosis
- Cleveland Clinic: Hereditary Spherocytosis
- StatPearls (NCBI Bookshelf): Hereditary Spherocytosis
- Polizzi A, et al. Overview on Hereditary Spherocytosis Diagnosis. Int J Lab Hematol, 2025
- Wang Y, et al. A novel variant in the SPTB gene underlying hereditary spherocytosis. BMC Med Genomics, 2024
Further reading
- Normal blood test ranges
- Abnormal blood test results
- A full blood panel
- CBC versus CMP blood tests
- The leukemia blood test
Understand your lab results with AI DiagMe
Get your results interpreted in minutes
If a blood test has flagged anemia or signs of red cell breakdown, it helps to know what each value means before your appointment. AI DiagMe reads your laboratory results — a complete blood count, reticulocyte count, bilirubin, LDH or haptoglobin — and turns them into a clear, easy-to-read explanation. It is built to help you understand your results and prepare better questions for your doctor; it does not diagnose disease and does not replace your medical team.
{kind=link}