


















An iron studies panel is a group of blood tests that, read together, show how much iron your body has in storage, how much is circulating right now, and how well it is being carried around. No single number tells the whole story, which is exactly why these tests are ordered as a set. This guide explains what an iron studies panel measures, what each marker means in plain language, and how the values fit together to point toward iron deficiency, inflammation or iron overload. You will also learn how to read the most confusing result combinations, how to prepare for the test, and when results are worth discussing with a doctor.
What is an iron studies panel?
An iron studies panel (sometimes called an iron panel or iron profile) is a set of blood tests that assess your body’s iron status from several angles at once. Iron is essential for making hemoglobin, the part of red blood cells that carries oxygen, so both too little and too much iron can affect your health.
A typical panel reports four to five values: serum iron, ferritin, transferrin and/or total iron-binding capacity (TIBC), and transferrin saturation. According to MedlinePlus, these tests are used to check whether iron levels are too low, to help diagnose different types of anemia, and to check whether iron is building up too high, a sign of conditions such as hemochromatosis.
Doctors often order an iron studies panel after a routine complete blood count (CBC) shows small, pale red blood cells, or when someone reports tiredness, shortness of breath, hair thinning or unusual cravings. It may also be requested to monitor a known iron condition over time. The panel does not, on its own, explain why iron is high or low; it maps out the iron picture so a clinician can look for the cause.
The markers in an iron studies panel, one by one
Each test in the panel reflects a different part of how your body handles iron. Reading them individually first makes the combined picture far easier to understand.
Serum iron
Serum iron measures the amount of iron travelling in your blood at the moment the sample is taken. Almost all of this iron is attached to a transport protein rather than floating freely.
The catch is that serum iron is a snapshot, not a stable measurement. It rises and falls across the day and after meals or supplements, so a single value can be misleading. That is one reason it is always interpreted alongside ferritin, TIBC and saturation rather than alone. You can read more in our dedicated guide to serum iron and what high and low levels mean.
Ferritin
Ferritin is a protein that stores iron inside your cells and releases it when needed. Your blood ferritin level reflects how much iron you have in reserve, which makes it the single most useful marker of your body’s iron stores.
Ferritin is also relatively steady, so it is not thrown off by a recent meal the way serum iron can be. There is an important twist, though: ferritin is an acute-phase reactant, meaning it rises during inflammation, infection or liver problems. A normal or high ferritin can therefore sometimes hide low iron stores. We cover the two directions in detail in our guides to low ferritin and high ferritin levels, as well as the broader role of ferritin as a health marker.
Transferrin and TIBC
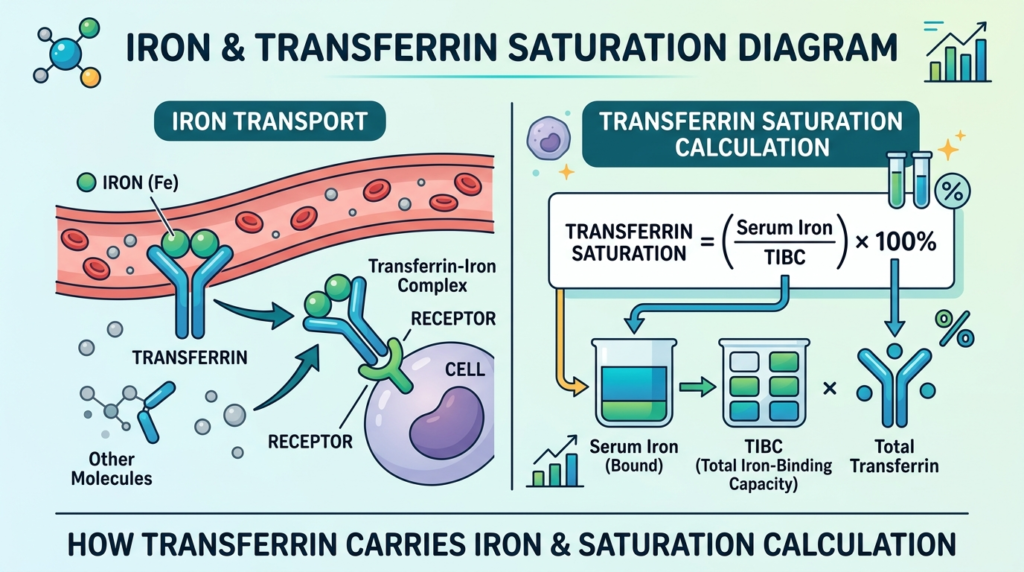
Transferrin is the main protein that carries iron through your blood, produced mostly by the liver. Its level moves in the opposite direction to your iron stores: when iron is low, your body makes more transferrin to capture as much iron as possible; when iron is high, it makes less. See our explainer on transferrin and its role in iron transport for more.
Total iron-binding capacity (TIBC) is a closely related number. It estimates how much iron your blood could carry if all the transferrin were full, so it largely mirrors transferrin. A high TIBC usually points to depleted iron stores, while a low or normal TIBC fits with iron overload or chronic disease. Our article on a high total iron-binding capacity walks through the causes. Some panels also list UIBC (unsaturated iron-binding capacity), the unused part of that capacity; TIBC is simply serum iron plus UIBC.
Transferrin saturation
Transferrin saturation, often shortened to TSAT, is the percentage of your transport protein that is actually carrying iron. It is calculated by dividing serum iron by TIBC and multiplying by 100.
In healthy adults, transferrin is normally about one-third saturated. A low saturation suggests there is not enough iron to fill the carriers, while a high saturation suggests there is more iron than the body needs. Because it combines two values, saturation is often a more telling marker than serum iron alone. Our guide on iron saturation, its levels and causes explains the practical range.
The table below summarises what each marker reflects. Reference ranges are approximate and vary by laboratory, sex and age, so always compare your result against the range printed on your own report.
| Marker | What it reflects | Typical adult range | Good to know |
|---|---|---|---|
| Serum iron | Iron circulating in your blood right now | About 60–170 µg/dL (≈11–30 µmol/L) | Swings during the day and after meals |
| Transferrin | The protein that carries iron | About 200–360 mg/dL | Made by the liver; rises when stores are low |
| TIBC | How much iron your blood could carry | About 250–450 µg/dL | Mostly mirrors transferrin |
| UIBC | The unused part of that capacity | Varies by lab | TIBC = serum iron + UIBC |
| Transferrin saturation | Percentage of carriers holding iron | About 20–50% | Serum iron ÷ TIBC × 100 |
| Ferritin | Iron kept in storage | Women ≈15–150 ng/mL, men ≈30–400 ng/mL | Best single marker of stores; rises with inflammation |
How to read your iron studies panel results together
The real value of an iron studies panel comes from the pattern across the markers, not any one figure. Three common patterns cover most situations, and recognising them makes your report much less intimidating.
In iron deficiency, your stores are running out. Ferritin is low, serum iron is low, the body ramps up transferrin so TIBC is high, and transferrin saturation is low. This is the classic picture behind iron deficiency anemia, which often shows up first as small, pale red blood cells, or a low MCV on a complete blood count.
In inflammation or anemia of chronic disease, the body locks iron away inside storage cells even though total iron may be adequate. Serum iron is low, but ferritin is normal or high because inflammation pushes it up, and TIBC tends to be low or normal. An inflammatory marker such as C-reactive protein (CRP) is often raised at the same time, which is a useful clue.
In iron overload, there is too much iron. Serum iron is high, ferritin is high, TIBC is low or normal, and transferrin saturation is high, sometimes markedly so. This is the pattern seen in conditions such as hemochromatosis, where the body absorbs and stores more iron than it should.
The table below lines up these patterns side by side. It is a guide to typical findings, not a diagnosis; only a clinician can interpret your results in the context of your symptoms and history.
| Pattern | Serum iron | Ferritin | TIBC / transferrin | Saturation |
|---|---|---|---|---|
| Iron deficiency | Low | Low | High | Low |
| Inflammation / chronic disease | Low | Normal or high | Low or normal | Low or normal |
| Iron overload (e.g. hemochromatosis) | High | High | Low or normal | High |
| Healthy iron stores | Normal | Normal | Normal | Normal |
When the numbers don’t seem to add up
Plenty of real reports do not fall neatly into one column, and this is where people most often feel confused. A few mismatches are common and have logical explanations.
Low serum iron but normal ferritin. Because serum iron fluctuates so much during the day, a single low reading can simply reflect timing rather than true depletion. If ferritin (the stores marker) is comfortably normal, your overall iron status is usually reassuring. Saturation and TIBC help settle the question.
High ferritin but normal or low saturation. This combination usually points to inflammation rather than iron overload. Ferritin rises as part of the body’s response to infection, injury, obesity or liver issues, so a raised ferritin with an ordinary saturation often reflects an inflammatory state, not extra iron. In true overload, ferritin and saturation tend to rise together.
A normal panel despite ongoing symptoms. Tiredness, hair changes and poor concentration have many possible causes beyond iron, including thyroid problems, vitamin B12 deficiency and sleep issues. A normal iron studies panel helps rule iron out, but it does not rule out everything, so persistent symptoms still deserve follow-up.
Borderline ferritin. Levels just above the lower limit can still mean low functional iron for some people, especially if symptoms are present. This grey zone is one reason results are best reviewed alongside the full panel and your clinical picture rather than judged on a single threshold.
How an iron studies panel is done and how to prepare
The test itself is a standard blood draw, usually a single sample taken from a vein in your arm. The same sample can supply all the values in the panel, including the calculated ones such as TIBC and saturation.
Preparation matters more here than for many blood tests, because serum iron is sensitive to timing and food. As a result, iron studies are ideally collected in the morning after an overnight fast, when serum iron is typically at its highest and least affected by recent meals. Iron supplements can also raise serum iron temporarily, so labs often advise pausing them beforehand. Always follow the specific instructions from the team that ordered your test, as protocols differ.
A few practical points help you get a reliable result:
- Ask whether you should fast and for how long, since requirements vary by lab.
- Mention any iron tablets, multivitamins or recent infusions you have taken.
- Tell the team about recent illness or infection, which can push ferritin up.
- If you can, book a morning slot to reduce the effect of daily fluctuation.
Results are often available within a day or two, though exact turnaround depends on the laboratory.
When to see a doctor about your iron results
An iron studies panel is a screening and monitoring tool, not a verdict, and most out-of-range values are manageable once the cause is found. Still, some situations warrant prompt medical attention rather than waiting.
Consider contacting a healthcare professional if you notice any of the following:
- Marked tiredness, breathlessness, dizziness or a racing heartbeat that limits daily life.
- Ongoing low iron despite eating iron-rich foods, which may signal hidden blood loss that needs investigating.
- A very high ferritin or transferrin saturation, particularly with joint pain, abdominal pain or a family history of hemochromatosis.
- Iron deficiency in a man or a postmenopausal woman, where the source of loss should always be checked.
- Any new, severe or unexplained symptom alongside abnormal results.
Whatever your numbers show, the next step is a conversation, not self-treatment. Iron supplements can be unhelpful or even harmful if iron is normal or high, so changes are best guided by a clinician who can see the full panel and your history.
Glossary
- Acute-phase reactant: A protein, such as ferritin or CRP, whose blood level rises during inflammation or infection.
- Anemia of chronic disease: A type of anemia caused by long-term illness or inflammation that traps iron in storage rather than a true lack of iron.
- CBC (complete blood count): A common blood test counting red cells, white cells and platelets, often the first clue to iron problems.
- Ferritin: A protein that stores iron inside cells; its blood level reflects your iron reserves.
- Hemochromatosis: A condition in which the body absorbs and stores too much iron over time.
- Serum iron: The amount of iron circulating in your blood at the moment of the test.
- TIBC (total iron-binding capacity): An estimate of how much iron your blood could carry if all transferrin were full.
- Transferrin: The main protein that transports iron through the bloodstream.
- Transferrin saturation (TSAT): The percentage of transferrin currently carrying iron, calculated from serum iron and TIBC.
- UIBC (unsaturated iron-binding capacity): The unused portion of iron-carrying capacity; serum iron plus UIBC equals TIBC.
Frequently asked questions
Is ferritin the same as iron?
No, although they are closely related. Serum iron measures the iron travelling in your blood right now, while ferritin reflects the iron held in storage inside your cells. Because serum iron rises and falls throughout the day, ferritin is generally the more reliable single marker of how much iron you have in reserve. The two can also disagree: you can have a temporarily low serum iron with normal stores, or a raised ferritin from inflammation while circulating iron is unremarkable. That is precisely why an iron studies panel looks at both, plus transferrin saturation and TIBC, rather than relying on one figure.
Do I need to fast before an iron studies panel?
Often, yes. Serum iron is sensitive to food and to the time of day, so many laboratories ask for a morning sample after an overnight fast to get a more consistent reading. Iron supplements can also raise serum iron for a while, so you may be asked to pause them beforehand. The exact instructions vary, however, so follow the guidance from the team that ordered the test. If you were not given any specific advice, it is reasonable to ask whether fasting is needed and whether to hold your supplements.
What does it mean if my iron is low but my ferritin is normal?
This is a common and usually reassuring combination. Serum iron naturally fluctuates during the day, so a single low value may simply reflect timing rather than depleted stores. Ferritin, which measures your reserves, is more stable, so a normal ferritin generally suggests your overall iron status is adequate. Transferrin saturation and TIBC help confirm the picture. If symptoms persist or ferritin is only borderline, it is still worth discussing with a clinician, since the “normal” range is broad and the right level can vary from person to person.
Can iron levels change from day to day?
Serum iron certainly can, and even within the same day. It is typically higher in the morning and lower later on, and it can shift after meals or iron tablets. This day-to-day and hour-to-hour variation is one of the main reasons serum iron is never interpreted on its own. Ferritin and TIBC are far steadier, so they give a more dependable view of your iron status over time. Standardising the conditions of the test, such as a morning fasting draw, helps reduce this variability.
Should I worry if one value is flagged out of range?
Usually not on its own. Laboratory ranges are statistical guides, and a single slightly out-of-range value is common and often harmless, especially for a fluctuating marker like serum iron. What matters is the overall pattern across the panel, combined with how you feel and your medical history. A clinician reads the markers together before drawing any conclusion. If several values point the same way, or a result is markedly abnormal, that is a clearer signal to investigate further.
What is the difference between TIBC and transferrin saturation?
They describe related but distinct things. TIBC estimates the total capacity of your blood to carry iron, which largely reflects how much transferrin you have. Transferrin saturation, by contrast, tells you how much of that capacity is actually being used, expressed as a percentage and calculated from serum iron and TIBC. A simple way to picture it: TIBC is the size of the fleet of carriers, while saturation is how full those carriers are. In iron deficiency the fleet grows (high TIBC) but runs nearly empty (low saturation); in iron overload the fleet may shrink (low or normal TIBC) yet runs very full (high saturation).
Sources
- Iron Tests — MedlinePlus (U.S. National Library of Medicine)
- Iron deficiency anaemia — NHS
- Iron-Binding Capacity — StatPearls, NCBI Bookshelf (NIH)
Further reading
- Ferritin: understanding this blood marker for your health
- Serum iron test: how to read high, low and normal levels
- Understanding a high total iron-binding capacity
- Iron saturation explained: levels and causes
- Hemochromatosis treatments: a practical guide
Understand your lab results with AI DiagMe
Reading an iron studies panel means weighing several numbers at once: your iron stores (ferritin), the iron circulating now (serum iron), your carrying capacity (TIBC and transferrin), and how full those carriers are (transferrin saturation). It is easy to fixate on one flagged value and miss the pattern that actually matters. AI DiagMe helps you make sense of these results together and put them in context, in plain language and within minutes. It is designed to help you understand your report, not to diagnose you or replace your doctor, so you walk into your next appointment better informed.
➡️ Get your results interpreted in minutes
{kind=link}