


















A diabetes blood test is the simplest, most reliable way to find out whether your blood sugar sits in a healthy range or has started to drift too high. If you have just had blood drawn, or your doctor mentioned screening you for diabetes, you are probably looking at three confusing words on your results: glucose, HbA1c, and insulin. This guide explains what each one measures, how the main tests differ, and exactly what the numbers mean. You will see the normal, prediabetes, and diabetes cut-offs side by side, a chart that converts HbA1c into an average glucose figure, and clear advice on how to prepare and when to call a doctor. None of this replaces a clinician, but it will help you read your own report with far more confidence.
What a diabetes blood test measures
A diabetes blood test does not look at one single thing. Depending on the test your doctor orders, it measures one or more of three markers that, together, describe how your body handles sugar.
The first is glucose, the sugar your cells burn for energy. A glucose result is a snapshot: it tells you how much sugar was in your blood at the exact moment the sample was taken. You can learn more in our guide to blood glucose levels, and note that a glucose reading is also one of the values on a comprehensive metabolic panel.
The second is HbA1c, also called glycated hemoglobin or A1C. Sugar in your blood sticks to hemoglobin, the protein that carries oxygen inside red blood cells. Because those cells live for about three months, HbA1c reflects your average blood sugar over roughly 8 to 12 weeks. It is the long-view marker.
The third is insulin, the hormone your pancreas releases to move glucose out of the blood and into cells. An insulin blood test is less common than the other two and is used to study how your body responds to sugar rather than to diagnose diabetes on its own.
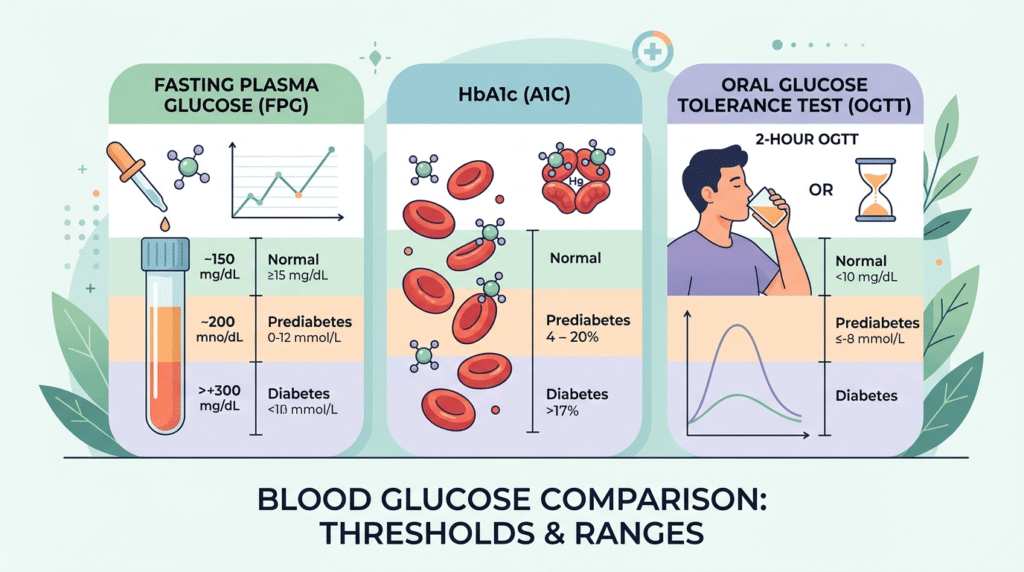
The main diabetes blood tests, side by side
Four tests do almost all of the work in diagnosing diabetes. They are accepted by major health bodies, including the U.S. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and the Centers for Disease Control and Prevention (CDC). Here they are with their diagnostic cut-offs.
| Test | Normal | Prediabetes | Diabetes |
|---|---|---|---|
| Fasting plasma glucose (FPG) | Below 100 mg/dL (5.6 mmol/L) | 100–125 mg/dL (5.6–6.9 mmol/L) | 126 mg/dL (7.0 mmol/L) or higher |
| HbA1c (A1C) | Below 5.7% | 5.7%–6.4% | 6.5% or higher |
| Oral glucose tolerance test (2-hour) | Below 140 mg/dL (7.8 mmol/L) | 140–199 mg/dL (7.8–11.0 mmol/L) | 200 mg/dL (11.1 mmol/L) or higher |
| Random plasma glucose | — | — | 200 mg/dL (11.1 mmol/L) or higher, with symptoms |
One result is rarely the final word. Apart from a clearly very high reading combined with classic symptoms, a diagnosis usually needs a second abnormal result, either by repeating the same test or running a different one on another day. If you want help making sense of the layout and the “H” or “L” flags on your sheet, see our guide on how to read your blood test results.
Fasting plasma glucose (FPG)
This test measures your sugar after at least eight hours with nothing to eat or drink except water. It is usually done first thing in the morning. A fasting blood glucose result is straightforward and inexpensive, which is why it is so widely used. Its main limitation is that it depends on you fasting correctly, and a single high value can be nudged by short-term factors such as illness, a poor night’s sleep, or significant stress. That is part of why one raised reading is usually repeated rather than acted on right away.
HbA1c (glycated hemoglobin)
HbA1c needs no fasting and can be taken at any time of day, which makes it convenient. Because it is an average, it smooths out the daily ups and downs that a single glucose reading would catch. The trade-off is that anything affecting your red blood cells, such as certain anemias or inherited hemoglobin variants, can make the result less reliable. Our article on the HbA1c normal range and target levels goes deeper into what the percentage means.
Oral glucose tolerance test (OGTT)
For this test you fast, have a baseline glucose drawn, drink a measured sugary liquid (usually 75 grams of glucose), then have blood taken two hours later. The OGTT shows how efficiently your body clears a sugar load. It takes longer and is more demanding than the others, so it is reserved for specific situations, such as pregnancy or borderline results. It is also useful when an HbA1c may be unreliable, because it measures glucose directly rather than relying on red blood cells. The downside is the time commitment and the sugary drink, which some people find unpleasant.
Random plasma glucose
A random test is taken at any time, regardless of when you last ate. On its own it cannot rule diabetes in or out, but a reading of 200 mg/dL (11.1 mmol/L) or higher in someone with classic symptoms, such as intense thirst and frequent urination, points strongly to diabetes and prompts confirmation.
From HbA1c to average glucose: the conversion chart
One of the most common questions is how a percentage relates to the glucose numbers people see on a home meter. The American Diabetes Association publishes a formula that turns HbA1c into an estimated average glucose (eAG). The table below shows the key reference points.
| HbA1c | Estimated average glucose (mg/dL) | Estimated average glucose (mmol/L) |
|---|---|---|
| 5% | 97 | 5.4 |
| 6% | 126 | 7.0 |
| 6.5% | 140 | 7.8 |
| 7% | 154 | 8.6 |
| 8% | 183 | 10.2 |
| 9% | 212 | 11.8 |
| 10% | 240 | 13.4 |
A practical note on units: in the United States, HbA1c is reported as a percentage. In the United Kingdom and much of the rest of the world it appears in mmol/mol, where 6.0% equals 42 mmol/mol and 6.5% equals 48 mmol/mol. If your report uses one system and your reading uses the other, the figures above can help you bridge the two.
What the numbers mean: normal, prediabetes, and diabetes
Reading your result is mostly about knowing which band it falls into.
Normal means your sugar handling looks healthy. A fasting glucose under 100 mg/dL and an HbA1c under 5.7% are both in this range.
Prediabetes is the warning zone. Your blood sugar is higher than normal but not yet in the diabetes range. A fasting glucose of 100–125 mg/dL is sometimes called impaired fasting glucose, and a two-hour OGTT of 140–199 mg/dL is called impaired glucose tolerance. Prediabetes is common, often silent, and frequently reversible with changes to diet, weight, and activity. It often goes hand in hand with insulin resistance, where the body stops responding well to its own insulin.
Diabetes is diagnosed when the markers cross the upper thresholds and are confirmed. For the full picture of types, causes, and treatment, see our overview of how diabetes is diagnosed and managed.
Because the different tests do not always agree, a normal fasting glucose paired with a prediabetes-range HbA1c is not unusual. Clinicians expect this and look at the whole picture rather than a single figure.
What happens after an abnormal result is just as important as the number itself. For prediabetes, the usual next step is a recheck within a year alongside lifestyle support, since the trend over time matters more than one reading. For a result in the diabetes range, your doctor will confirm it and then work out which type of diabetes you have, because that decides treatment. Younger people, those who lose weight quickly, or anyone who is acutely unwell may have further tests to check for type 1 diabetes rather than type 2. In every case, the result is a starting point for a conversation, not a verdict you have to interpret alone.
Where insulin tests fit in (and what they don’t tell you)
Insulin tests answer a different question from glucose and HbA1c. Rather than asking “how high is your sugar,” they ask “how hard is your pancreas working to keep it down.”
A fasting insulin result, measured after an overnight fast, is often combined with fasting glucose to calculate a score called HOMA-IR, which estimates insulin resistance. Our HOMA-IR guide walks through how that calculation works. A high fasting insulin can flag a body straining to manage sugar well before glucose levels rise.
Two related tests sometimes appear on the same workup. C-peptide shows how much insulin your own body is producing, and autoantibody tests look for the immune markers seen in type 1 diabetes. Together these help distinguish type 1 from type 2 when the picture is unclear.
The key point is that fasting insulin is not a stand-alone diabetes test. There is no single insulin cut-off that diagnoses the condition, and reference ranges vary between laboratories. It adds context; it does not replace glucose or HbA1c.
Insulin testing has drawn more interest in recent years because insulin resistance can build for a long time before glucose rises, so the idea of catching trouble earlier is appealing. Even so, major guidelines still rely on glucose and HbA1c for diagnosis, and a fasting insulin result is best read with a clinician who can weigh it against your other markers and your overall risk rather than in isolation.
How to prepare for a diabetes blood test
Good preparation makes your results more accurate. The steps depend on which test you are having.
- For a fasting glucose or an OGTT, do not eat or drink anything except water for at least eight hours beforehand. Black coffee and tea without milk or sugar are usually fine to skip too, since they can nudge readings; when in doubt, stick to water.
- For an HbA1c, you do not need to fast at all. You can eat and drink normally and book the test for any time of day.
- Take your usual medications unless your doctor tells you otherwise, and mention everything you take, since some drugs affect blood sugar.
- Stay hydrated with water, which also makes the blood draw easier.
- Bring a list of your medications and any symptoms, and tell the lab if you are pregnant or have a condition affecting your red blood cells.
- Avoid heavy exercise, alcohol, and being acutely unwell right before a fasting test, as each can temporarily move your glucose; if you are ill, it is often worth rescheduling a screening test.
A single sugary meal the day before will not turn a healthy person diabetic, but it can lift a random or post-meal glucose reading, which is one more reason fasting and HbA1c tests are preferred for diagnosis.
Special situations: pregnancy, children, and older adults
Diabetes testing is not one-size-fits-all.
During pregnancy, doctors screen for gestational diabetes, usually between 24 and 28 weeks, often with a glucose challenge followed by an OGTT if needed. The cut-offs differ from the standard ones, and the goal is to protect both parent and baby. Our guide to blood tests during pregnancy explains what is checked and when.
In children, especially when symptoms come on quickly, type 1 diabetes is a stronger consideration, and testing often includes glucose plus antibody and C-peptide checks.
In older adults, HbA1c can be skewed by other conditions, so a clinician may lean on glucose tests or interpret targets more flexibly. The takeaway is that your age and circumstances shape both which test is best and how the result is read.
When to see a doctor: warning signs you shouldn’t ignore
Most diabetes is found through routine screening, not a crisis. Still, some symptoms warrant prompt medical attention rather than waiting for a scheduled test:
- Constant thirst and a dry mouth that does not ease
- Needing to urinate far more often than usual, including overnight
- Unexplained weight loss
- Extreme tiredness or blurred vision
- Slow-healing cuts or frequent infections
Seek urgent care if you have nausea and vomiting, deep or rapid breathing, fruity-smelling breath, confusion, or abdominal pain. These can signal a dangerous complication called diabetic ketoacidosis, which is often accompanied by ketones in your urine. It needs immediate treatment. When symptoms like these appear, do not rely on a home test to decide what to do — contact a healthcare professional straight away.
Glossary
- eAG (estimated average glucose): an average glucose figure, in mg/dL or mmol/L, calculated from your HbA1c so you can compare it to home-meter readings.
- Fasting plasma glucose (FPG): a blood glucose measurement taken after at least eight hours without food, used to screen for and diagnose diabetes.
- Gestational diabetes: raised blood sugar first found during pregnancy, screened for with a glucose challenge or tolerance test.
- Glycated hemoglobin (HbA1c, A1C): the share of hemoglobin coated with sugar, reflecting average blood glucose over the past 8 to 12 weeks.
- Impaired fasting glucose: a fasting glucose in the prediabetes range (100–125 mg/dL), signalling higher-than-normal sugar.
- Impaired glucose tolerance: a two-hour OGTT result in the prediabetes range (140–199 mg/dL).
- Insulin: the hormone made by the pancreas that moves glucose from the blood into cells for energy.
- Insulin resistance: a state in which cells respond poorly to insulin, so the body must produce more to keep sugar in check.
- Oral glucose tolerance test (OGTT): a test that measures glucose before and two hours after a measured sugary drink.
- Prediabetes: blood sugar that is higher than normal but below the diabetes threshold, and often reversible.
Frequently asked questions
Can a routine blood test detect diabetes?
Only if it includes the right marker. A standard panel often contains a glucose reading, which can flag a problem, and many checkups add an HbA1c. But not every “routine” blood test measures blood sugar. If you want to know your diabetes risk, ask specifically for a fasting glucose or an HbA1c rather than assuming a general blood test covers it. If a result is borderline or abnormal, your doctor will usually arrange a second test to confirm before making any diagnosis.
Do I need to fast for an HbA1c test?
No. The HbA1c test reflects your average blood sugar over the past two to three months, so a single meal or drink beforehand does not change the result. You can have it taken at any time of day without fasting. Fasting is only required for a fasting plasma glucose test or for the start of an oral glucose tolerance test. If your doctor is ordering several tests at once, such as cholesterol alongside your sugar markers, they may still ask you to fast for those other tests.
How often should I get a diabetes blood test?
It depends on your risk. Many guidelines suggest screening from around age 35 for adults, repeating roughly every three years if results are normal. People with extra risk factors, such as excess weight, a family history of diabetes, high blood pressure, or a past pregnancy with gestational diabetes, may be tested earlier and more often. If you have prediabetes, your doctor will usually recheck your levels every year. Your own schedule should be set with a healthcare professional who knows your history.
Can diabetes go undetected on a blood test?
Sometimes. A single test can miss early or borderline cases, which is one reason confirmation testing exists. The HbA1c test in particular can be unreliable in people with certain anemias, recent blood loss, or inherited hemoglobin variants, occasionally reading falsely low. Different tests can also disagree, so a normal fasting glucose does not always rule out a problem an HbA1c or OGTT would catch. If you have clear symptoms but a normal result, tell your doctor, who may repeat or switch tests.
Does eating sugar before the test affect the results?
For a random or post-meal glucose reading, yes, a sugary meal can temporarily raise the number. For a fasting glucose test, eating breaks the fast and invalidates the result, which is why you must avoid food beforehand. The HbA1c is barely affected by any single meal because it is a long-term average. Importantly, one indulgent meal does not cause diabetes, and it will not create a true diabetes diagnosis if your underlying sugar handling is healthy.
What’s the difference between a finger-prick test and a lab blood test?
A finger-prick test, like the ones on home meters, gives a quick snapshot and is excellent for day-to-day monitoring. For diagnosing diabetes, however, a sample drawn from a vein and analysed in an accredited laboratory is the standard, because it is more precise and consistent. A finger-prick result that looks high is a good reason to arrange a proper lab test rather than a diagnosis in itself.
Sources
- Diabetes Tests & Diagnosis — National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)
- Diabetes Testing — Centers for Disease Control and Prevention (CDC)
- Diabetes: Diagnosis and treatment — Mayo Clinic
Further reading
- Fasting blood glucose: your complete guide to interpretation
- HbA1c normal range: meaning and target levels
- Insulin blood test: understanding your levels
- Glucose levels: causes, symptoms, and treatments
- Diabetes: causes, symptoms, and treatments
Understand your lab results with AI DiagMe
Once your diabetes blood test comes back, a page of numbers can still feel like a puzzle. AI DiagMe helps you make sense of markers such as fasting blood sugar (fasting glucose), long-term sugar control (HbA1c), and how your body handles insulin, turning the figures into plain-language context. It is built to help you understand your results and prepare better questions for your appointment, not to diagnose you or replace your doctor. If you have a recent report in hand, let AI DiagMe walk you through what each value means.
➡️ Get your results interpreted in minutes
{kind=link}