


















An adrenal panel is a group of blood tests that measures the main hormones your adrenal glands make, most often cortisol, adrenocorticotropic hormone (ACTH), aldosterone, and dehydroepiandrosterone sulfate (DHEA-S). If your doctor ordered one, it usually means they want to check how well these two small glands above your kidneys are working. Seeing several unfamiliar names and numbers on one report can feel confusing, especially when a value is flagged high or low. This guide explains what each marker does, how the results connect to each other, and what common high and low patterns can point to. You will also learn how to prepare for the test and when an abnormal value is worth discussing with a clinician. For the basics of any lab report, our guide to reading blood test results is a helpful starting point.
What is an adrenal panel?
An adrenal panel is not a single fixed test. It is a set of measurements your doctor chooses based on your symptoms. Most panels include a few core hormones, and the lab may add others to answer a specific question.
Doctors order an adrenal panel for several reasons. You might have symptoms that suggest too much or too little of an adrenal hormone, such as blood pressure that is hard to control, unusual fatigue, or changes in weight, mood, or skin. A panel may also follow up an adrenal nodule found by chance on a scan, or help monitor a condition that is already known. The exact markers depend on the question your doctor is trying to answer.
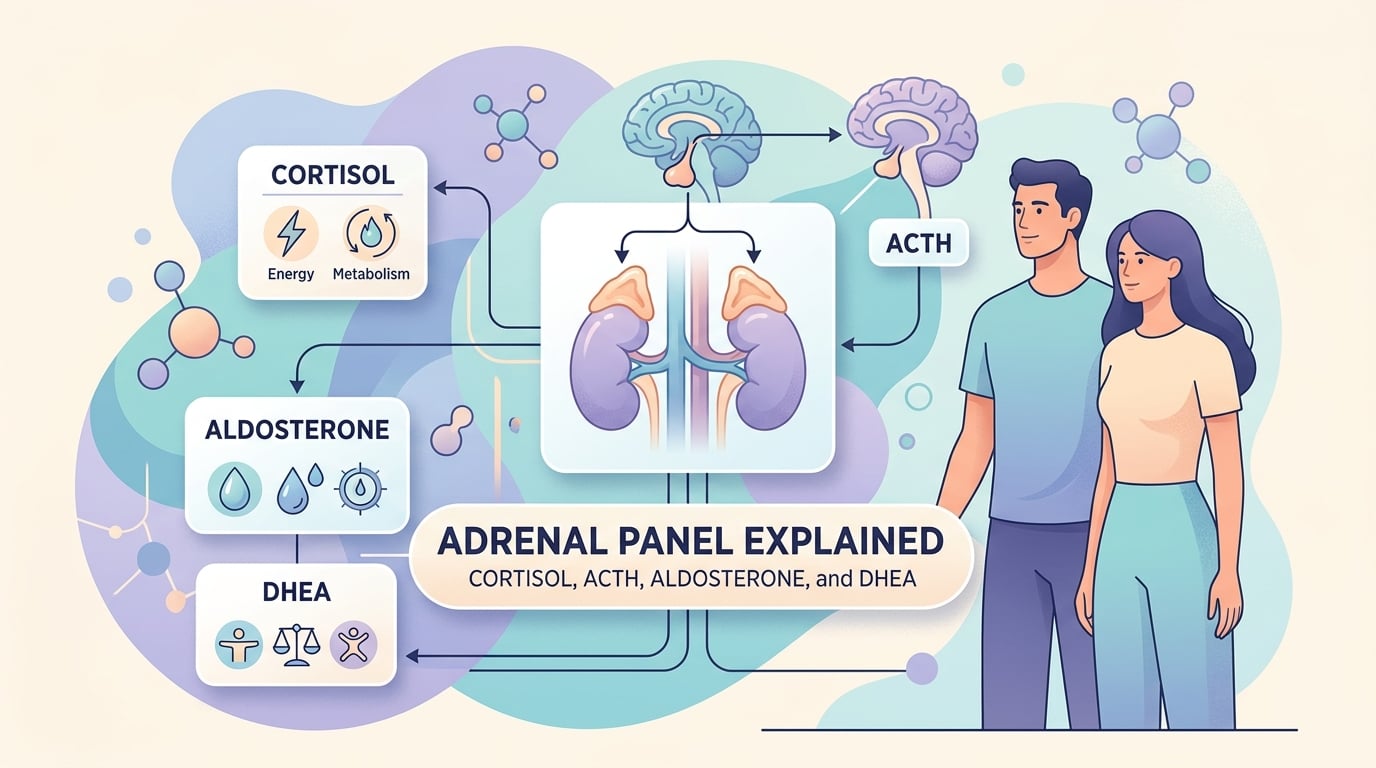
The adrenal glands sit on top of each kidney. They produce steroid hormones that help control your stress response, blood pressure, salt and water balance, blood sugar, and some sex-hormone precursors. An adrenal panel checks whether the levels of these hormones are too high, too low, or in the expected range.
Here is what each core marker measures:
| Marker | Short name | What it mainly reflects |
|---|---|---|
| Cortisol | Cortisol | The main stress and metabolism hormone |
| Adrenocorticotropic hormone | ACTH | The pituitary signal that tells the adrenals to make cortisol |
| Aldosterone | ALD | Salt, potassium, and blood-pressure control |
| DHEA-sulfate | DHEA-S | An adrenal androgen (a weak male-type hormone) |
Key points to keep in mind:
- One flagged value rarely gives a diagnosis on its own. Doctors read the markers together as a pattern.
- Timing matters: cortisol and ACTH change a lot across the day, so when your blood was drawn affects the result.
- Reference ranges vary between laboratories, so always compare your result with the range printed on your own report.
The four hormones in an adrenal panel
Each hormone in the panel tells a different part of the story. Understanding what they do makes the numbers easier to interpret.
Cortisol
Cortisol is often called the “stress hormone,” but it does far more than that. It helps regulate blood sugar, blood pressure, the sleep-wake cycle, and the body’s response to inflammation. Cortisol follows a daily rhythm: it is usually highest in the early morning and lowest late at night. Because of this, the time of the blood draw is part of the result. A morning sample is the most common. You can read more in our dedicated guide to the cortisol blood test. Sometimes a doctor adds a 24-hour urinary cortisol test to measure the total amount made over a full day.
ACTH (adrenocorticotropic hormone)
ACTH is made by the pituitary gland, a pea-sized gland at the base of the brain. Its job is to tell the adrenal glands to release cortisol. When cortisol is low, the pituitary makes more ACTH; when cortisol is high, it makes less. This back-and-forth is why ACTH and cortisol are almost always read together. Measuring both at the same time helps your doctor work out where a problem starts: in the adrenal glands themselves or higher up in the pituitary. Our guide to the ACTH blood test explains this signal in more detail.
Aldosterone
Aldosterone controls how much sodium your body keeps and how much potassium it lets go. By doing this, it helps regulate blood pressure and fluid balance. Aldosterone is part of a wider control loop called the renin-angiotensin-aldosterone system (RAAS), so labs often measure renin alongside it. Because aldosterone affects minerals, an adrenal panel may also include sodium and potassium. A separate aldosterone guide walks through this marker in plain language.
DHEA and DHEA-S
DHEA (dehydroepiandrosterone) and its stored form DHEA-S are weak androgens, meaning mild male-type hormones that the body can convert into other sex hormones. The adrenal glands are the main source of DHEA-S, which is why it appears on adrenal panels. Levels naturally peak in early adulthood and fall with age. An unexpectedly high or low DHEA-S can be a clue to adrenal activity. When androgen excess is being investigated, the panel may also include 17-OH progesterone, a marker linked to congenital adrenal hyperplasia (CAH). For a fuller look, see our explainer on DHEA levels.
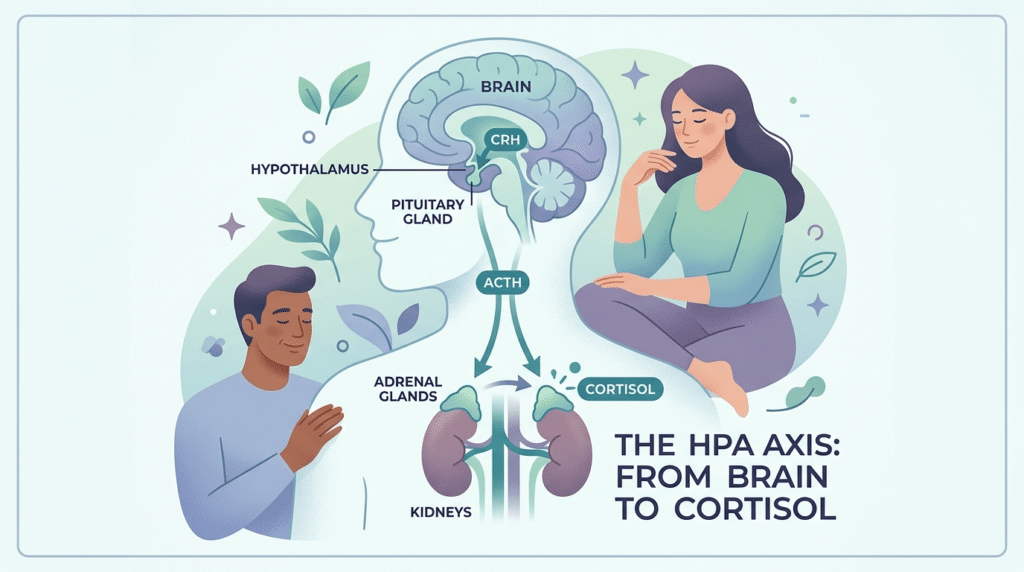
How the adrenal panel fits together: the HPA axis and RAAS
The markers in an adrenal panel are not independent. They sit inside two control loops, and knowing them is the key to reading paired results.
The first is the hypothalamic-pituitary-adrenal (HPA) axis. The brain’s hypothalamus signals the pituitary, the pituitary releases ACTH, and ACTH tells the adrenal glands to make cortisol. Rising cortisol then signals the brain to slow down, like a thermostat switching off the heat. This feedback loop is why a low cortisol can sit next to either a high or a low ACTH, and why the two together mean very different things.
The second loop is the RAAS, which manages blood pressure and salt. When blood pressure or sodium drops, the kidneys release renin, which sets off a chain that ends with the adrenal glands releasing aldosterone. Looking at aldosterone next to renin tells your doctor whether the adrenal glands are responding correctly or acting on their own.
This is why a panel is more useful than a single hormone. The numbers gain meaning from how they relate.
Reading your adrenal panel results: high and low patterns
A single result is a snapshot. Doctors interpret an adrenal panel by reading the markers as a pattern and by repeating tests when needed. The table below shows how cortisol and ACTH are often read together. It is a simplified guide, not a diagnosis.
| Cortisol | ACTH | What the pattern may point to | Typical next step |
|---|---|---|---|
| High | Low | An adrenal source making too much cortisol on its own, such as an adrenal nodule | Adrenal imaging and specialist review |
| High | High or normal | An ACTH-driven cause, such as a small pituitary tumor or, rarely, ACTH made elsewhere | Pituitary imaging and confirmatory tests |
| Low | High | Primary adrenal insufficiency (Addison’s disease), where the adrenals are underactive | ACTH stimulation test; check aldosterone, renin, electrolytes |
| Low | Low or normal | Secondary adrenal insufficiency, usually a pituitary problem or recent steroid use | Review of medicines and pituitary function |
High cortisol patterns
When cortisol stays high over time, doctors look for Cushing’s syndrome. The pattern in the table helps separate an adrenal cause from a pituitary one. A confirmed picture usually needs more than one test, because stress, illness, and certain medicines can raise cortisol temporarily. To confirm a true excess, doctors often use dynamic tests, such as a dexamethasone suppression test or a late-night cortisol measurement, rather than relying on a single daytime value. Our guide to Cushing’s syndrome explains the symptoms and confirmatory tests in more detail.
Low cortisol patterns
Low cortisol can mean the adrenal glands are underactive (primary) or that the pituitary is not sending enough ACTH (secondary). A high ACTH with low cortisol points toward the adrenal glands; a low or normal ACTH points higher up. The most common cause of low results, though, is the use of steroid medicines such as prednisone. When the picture is unclear, an ACTH stimulation test (also called a cosyntropin test) checks whether the adrenal glands can respond to a signal, which helps confirm or rule out adrenal insufficiency. We cover the morning picture in our article on low morning cortisol.
Aldosterone and DHEA-S patterns
High aldosterone with low renin can suggest primary aldosteronism (Conn’s syndrome), a treatable cause of high blood pressure that is often paired with low potassium. Doctors often look at the aldosterone-to-renin ratio rather than aldosterone alone, because the ratio shows whether the adrenal glands are acting independently of the body’s normal blood-pressure signals. Low aldosterone alongside low cortisol can occur in Addison’s disease. A low DHEA-S can also be an early clue to underactive adrenal glands, while a high DHEA-S may reflect an adrenal source of androgen excess seen in conditions such as polycystic ovary syndrome (PCOS) or, less often, an adrenal tumor.
Before your test: timing, prep, and what can skew results
A few simple steps help make your adrenal panel reliable.
- Timing. Cortisol and ACTH are usually drawn in the morning, often between 7 and 9 a.m., because that is when cortisol naturally peaks. Your lab may give you a specific window.
- Posture and activity. Aldosterone and renin are affected by whether you are lying down, sitting, or standing, and by recent exercise. The lab may ask you to rest before the draw.
- Medicines. Several common drugs change these results, including steroids, some blood-pressure medicines, oral contraceptives, and water pills (diuretics). Do not stop any medicine on your own; tell your doctor what you take so they can plan around it.
- Supplements. High-dose biotin (vitamin B7), found in many hair and nail products, can interfere with some hormone immunoassays. Mention it before testing.
- Stress and illness. Physical stress, infection, poor sleep, and even a difficult blood draw can nudge cortisol upward. One unusual result is often repeated before any conclusion is drawn.
Fasting is not always required for an adrenal panel, but follow the exact instructions your lab gives you.
“Adrenal fatigue”: what the science actually says
You may have seen the term “adrenal fatigue” used to explain tiredness, low energy, or burnout. It is worth being clear: adrenal fatigue is not a recognized medical diagnosis. According to the Endocrine Society, the adrenal glands do not become “worn out” or lose function because of everyday mental or physical stress.
That does not mean your symptoms are imaginary. Fatigue is real and has many genuine causes, from thyroid problems and anemia to poor sleep and depression. The point is that a standard adrenal panel is designed to detect true adrenal disease, such as Addison’s disease or Cushing’s syndrome, rather than a vague “fatigue” state. If you feel persistently exhausted, it is more useful to investigate the real cause with your doctor than to rely on at-home “adrenal fatigue” testing of uncertain value.
When to see a doctor: red flags and next steps
An adrenal panel is a tool to support a conversation with your clinician, not a substitute for one. See a doctor promptly if you have ongoing symptoms that could point to an adrenal problem, such as:
- Unexplained weight changes, easy bruising, a rounder face, or purple stretch marks (possible excess cortisol).
- Lasting fatigue with dizziness on standing, salt cravings, darkening of the skin, nausea, or unintended weight loss (possible adrenal insufficiency).
- High blood pressure that is hard to control, especially with low potassium (a reason to consider aldosterone testing).
Seek emergency care for an adrenal crisis, a rare but life-threatening event. Warning signs include sudden severe weakness, repeated vomiting, severe abdominal or leg pain, confusion, and a drop in blood pressure. This needs urgent treatment, so call emergency services rather than waiting.
For everyday results, remember that one out-of-range number is common and often harmless. Your doctor will look at the whole pattern, your symptoms, your medicines, and sometimes a repeat test before deciding what, if anything, it means.
Glossary
| Term | What it means |
|---|---|
| ACTH (adrenocorticotropic hormone) | A hormone from the pituitary gland that tells the adrenal glands to release cortisol. |
| Addison’s disease | Primary adrenal insufficiency: the adrenal glands themselves are underactive and make too little cortisol (and often aldosterone). |
| Adrenal glands | Two small glands on top of the kidneys that make cortisol, aldosterone, DHEA-S, and adrenaline. |
| Aldosterone | An adrenal hormone that controls sodium, potassium, and blood pressure. |
| Cortisol | The main adrenal hormone for stress response, blood sugar, and blood-pressure regulation; it follows a daily rhythm. |
| Cushing’s syndrome | A condition caused by too much cortisol over a long period. |
| DHEA-sulfate (DHEA-S) | A weak male-type hormone (androgen) made mainly by the adrenal glands. |
| HPA axis | The hypothalamic-pituitary-adrenal loop: brain to pituitary to adrenal glands, which controls cortisol. |
| Renin / aldosterone-to-renin ratio | Renin is a kidney signal; comparing aldosterone to renin helps spot conditions like primary aldosteronism. |
Frequently asked questions
Is there a “normal” cortisol level?
There is no single normal cortisol number. Because cortisol rises and falls across the day, the expected range depends on when your blood was drawn, usually morning versus evening, and on the laboratory doing the test. A morning value that looks “high” might be perfectly normal for that time of day. This is also why doctors rarely judge cortisol on one reading alone. They consider the time of the draw, your symptoms, and often a second test or a paired ACTH result before deciding whether anything is out of balance.
What does a high DHEA-sulfate result mean in women?
A raised DHEA-S in women points to higher adrenal androgen (male-type hormone) activity. Common reasons include polycystic ovary syndrome (PCOS), which can come with irregular periods, acne, or extra hair growth. Less often, a markedly high DHEA-S can suggest a condition affecting the adrenal glands, such as congenital adrenal hyperplasia or an adrenal tumor. The size of the increase matters, and a single mildly raised value is usually followed by repeat or additional tests rather than treated as a diagnosis. A clinician will interpret it alongside your other hormones and symptoms.
Can I check my cortisol at home with a saliva test?
At-home saliva kits exist, and late-night salivary cortisol is a tool doctors sometimes use to investigate Cushing’s syndrome, because cortisol should be very low at night. However, home tests vary in quality, and results still need a professional to interpret them in context. They are not a reliable way to diagnose vague tiredness or “adrenal fatigue.” If you are concerned about your cortisol, it is better to discuss testing with your doctor, who can order the right test at the right time and read it alongside your full picture.
What’s the difference between DHEA and DHEA-S on my report?
DHEA and DHEA-S are closely related. DHEA is the active form, while DHEA-S is the more stable, stored “sulfate” version that circulates in much larger amounts. Because DHEA-S levels stay steadier through the day and come almost entirely from the adrenal glands, labs usually measure DHEA-S rather than DHEA when assessing adrenal function. If your report shows one but not the other, that is normal. Both reflect adrenal androgen activity, and your doctor will choose whichever is most useful for the question being asked.
How long do adrenal panel results take?
Turnaround depends on the marker and the laboratory. Common hormones like cortisol and DHEA-S often come back within a few days, while specialized or send-out tests may take longer. Tests that involve timed samples, such as an ACTH stimulation test, can add time because the lab processes several draws. Your clinic can give you a realistic estimate for your specific panel. For a fuller explanation of what affects timing, see our guide on how long blood test results take.
Should I worry if one value on my adrenal panel is abnormal?
Usually not on its own. A single out-of-range result is common and can come from the time of day, recent stress, illness, medicines, or normal biological variation. Doctors expect this, which is why they read the markers together and often repeat an unusual value before acting on it. What matters more is the overall pattern and whether it fits your symptoms. The most helpful next step is to bring the report to your doctor, who can decide whether it needs follow-up or no action at all.
Sources
- Adrenal Hormones — Endocrine Society
- Adrenal Gland: Function and Disorders — Cleveland Clinic
- Cortisol Test — MedlinePlus (U.S. National Library of Medicine)
Further reading
- How to read blood test results: a simple guide
- Cortisol: a guide to understanding your blood test
- Female hormone panel: what your results mean
- Comprehensive metabolic panel: how to read it
- Cushing’s syndrome: symptoms, causes, treatments
Understand your lab results with AI DiagMe
Reading an adrenal panel is easier when you can see how cortisol, ACTH, aldosterone, and DHEA-sulfate (DHEA-S) fit together rather than as isolated numbers. AI DiagMe turns your blood, urine, or stool results into clear, plain-language explanations, so you arrive at your appointment knowing which questions to ask. It is built to help you understand your results, not to diagnose you, and it never replaces your doctor’s judgment.
➡️ Get your results interpreted in minutes


{kind=link}