


















A female hormone panel is a single blood test that checks several reproductive hormones at once, most often follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol, and prolactin. If you have just received these results and a value sits outside the reference range, it is normal to wonder what it means. One flagged number is rarely the whole story, because these hormones rise and fall across your cycle and work as a team. This guide explains what each hormone does, when in your cycle to test, and, most importantly, how to read the four results together. You will also find a pattern table that links common hormone profiles to what they can suggest, a plain-language glossary, and clear signs that it is time to see a doctor.
What is a female hormone panel?
A female hormone panel is a blood test that measures several hormones involved in the menstrual cycle and fertility from one sample. The core of most panels is four markers: FSH, LH, estradiol, and prolactin. Many labs add others, such as progesterone, total testosterone, thyroid-stimulating hormone (TSH), and anti-Müllerian hormone (AMH), depending on why the test was ordered.
These hormones are part of a feedback loop sometimes called the hypothalamic-pituitary-ovarian (HPO) axis. In plain terms, the brain (the hypothalamus and the pituitary gland) sends chemical signals to the ovaries, and the ovaries send signals back. FSH and LH come from the pituitary; estradiol comes from the ovaries; prolactin also comes from the pituitary.
A doctor may order a panel when periods are irregular, very heavy, or have stopped; when you have trouble conceiving; when symptoms suggest perimenopause or menopause; or when there are signs of high prolactin, such as milky nipple discharge. Because each result only makes sense in context, it helps to first understand how to read blood test results and what a reference range actually represents.
The four core hormones, one by one
Before looking at individual values, this quick-reference table summarises what each hormone reflects and when it is best measured.
| Hormone | Where it is made | What it mainly reflects | Best time to test |
|---|---|---|---|
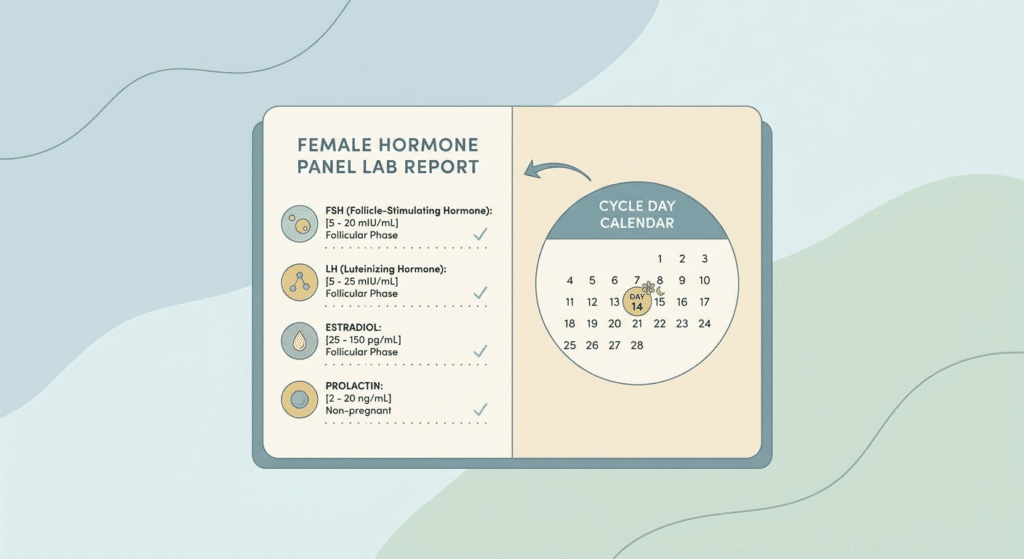
| FSH | Pituitary gland | Ovarian reserve and pituitary signalling | Cycle day 2–4 |
| LH | Pituitary gland | Ovulation timing; works alongside FSH | Cycle day 2–4 (baseline) or mid-cycle for the surge |
| Estradiol (E2) | Growing ovarian follicles | The main estrogen; follicle activity | Cycle day 2–4 |
| Prolactin | Pituitary gland | Milk production; can disturb periods when high | Morning, after resting |
Follicle-stimulating hormone (FSH)
FSH tells the ovaries to grow follicles, the small sacs that each contain an egg. Its level is often used as a rough marker of ovarian reserve, meaning how many eggs remain. When the ovaries become less responsive, the pituitary releases more FSH to push them along, so a high FSH can point to reduced reserve or the approach of menopause. A low FSH alongside low estradiol can instead suggest the signal from the brain is weak. You can explore this marker in depth in the dedicated guide on the FSH blood test.
Luteinizing hormone (LH)
LH works closely with FSH. Its job is to trigger ovulation: a sharp mid-cycle surge in LH causes a mature follicle to release its egg. This is the same surge that home ovulation predictor kits detect in urine. On a baseline blood test early in the cycle, a high LH compared with FSH (a raised LH-to-FSH ratio) is one feature that can accompany polycystic ovary syndrome. The full picture of this hormone is covered in the guide on the LH blood test.
Estradiol (E2)
Estradiol is the main and most active form of estrogen. It is made largely by the follicles as they grow, so it tends to rise through the first half of the cycle. Beyond fertility, estradiol supports bone strength and mood. A low estradiol that appears together with a high FSH is a classic combination seen around menopause. For more detail on values and what affects them, see the guide on estradiol.
Prolactin
Prolactin is best known for driving breast-milk production. Outside pregnancy and breastfeeding, a high level (called hyperprolactinemia) can quietly disturb the cycle, leading to irregular or absent periods and difficulty conceiving. Common reasons include stress, certain medicines, an underactive thyroid, and a benign pituitary growth called a prolactinoma. When a result comes back high, doctors usually look at the causes and the size of the rise, as explained in the guide on high prolactin levels.
When in your cycle should you test?
Timing matters more for a female hormone panel than for almost any other blood test, because levels swing across the month. Drawing blood on the wrong day can make a normal result look abnormal.
| Hormone | When to test | Why the timing matters |
|---|---|---|
| FSH, LH, estradiol | Cycle day 2–4 (often called “day 3”) | Levels sit at a stable baseline that can be compared with reference ranges |
| Progesterone | About day 21, or 7 days after ovulation | Shows whether ovulation happened that cycle |
| Prolactin | Morning, after resting | Prolactin rises with stress, exercise, and recent meals |
| AMH | Any day | Stays fairly steady across the cycle |
Day one is the first day of full bleeding. So “day 3” usually means the third day after your period starts. If your periods have stopped completely, the cycle-day rule no longer applies, and the panel can be drawn on any day.
If a doctor suspects a cause of extra male-type hormones, such as polycystic ovary syndrome, the panel may be widened. Tests like 17-OH progesterone and sex hormone-binding globulin (SHBG) help clarify how much hormone is active in the body rather than bound and inactive.
How to prepare for the test
Most female hormone tests do not require fasting. FSH, LH, estradiol, and prolactin can usually be measured whether or not you have eaten. Some laboratories ask you to fast when the panel is combined with glucose or cholesterol tests, so the simplest rule is to follow the instructions printed on your lab slip.
Prolactin is the one hormone that needs a little care. Its level can rise briefly with stress, vigorous exercise, a recent meal, or even breast stimulation, so the blood is best drawn in the morning after you have rested for a short while. If a first result is only mildly high, doctors often repeat it under calmer conditions before drawing any conclusions.
It also helps to tell the lab or your doctor a few things in advance:
- The day of your cycle, or that your periods have stopped.
- Any medicines you take. Hormonal birth control suppresses FSH, LH, and estradiol, and some medicines can raise prolactin.
- Whether you are pregnant or breastfeeding, which changes several of these values.
How to read your female hormone panel results
Two ideas make a female hormone panel far easier to understand. First, reference ranges depend on your cycle phase, your age, and the laboratory’s own method, so an “H” or “L” flag beside a number is a prompt to look closer, not a diagnosis. Second, and more important, these hormones are read together, not in isolation. The same FSH value can mean very different things depending on what estradiol, LH, and prolactin are doing.
The table below shows how the four markers tend to move together in common situations. It is a map for conversation with your doctor, not a self-diagnosis tool.
| Hormone pattern | What it can suggest |
|---|---|
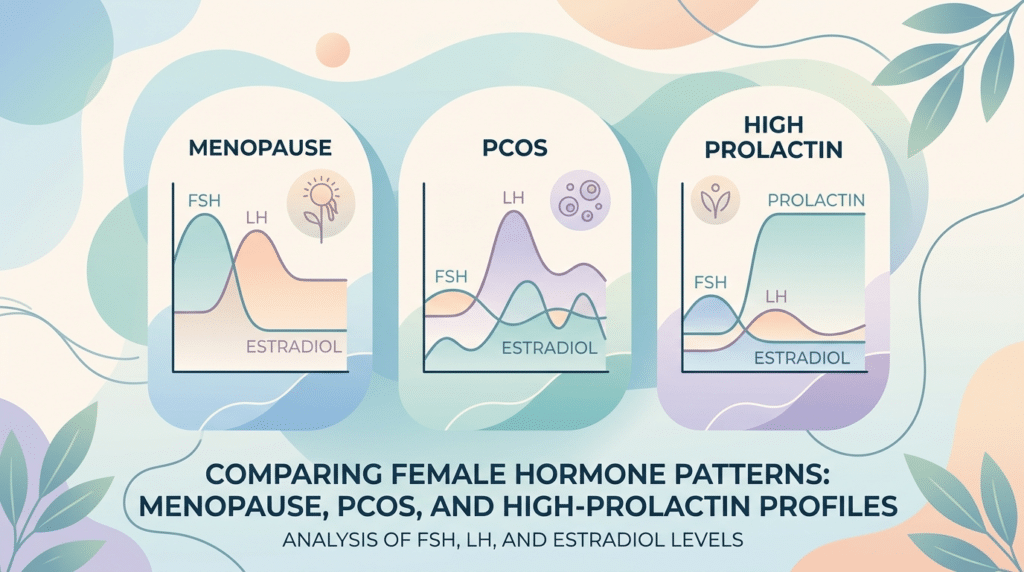
| High FSH with low estradiol (LH may also be high) | Menopause, perimenopause, or reduced ovarian reserve |
| Raised LH with a high LH-to-FSH ratio (testosterone may also be high) | A pattern often seen in polycystic ovary syndrome (PCOS) |
| High prolactin with normal or low FSH and LH | A pituitary cause, such as a prolactinoma, certain medicines, or an underactive thyroid |
| Low FSH, low LH, and low estradiol together | A hypothalamic cause, such as very low body weight, heavy training, or high stress |
| A mid-cycle spike in LH | Normal ovulation is approaching |
Because thyroid problems can copy many of the same symptoms and can also raise prolactin, doctors often check thyroid levels at the same time.
What different patterns can mean
A pattern pointing to menopause or perimenopause
As the ovaries wind down, they make less estradiol, and the pituitary responds by pushing out more FSH. A high FSH with a low estradiol is therefore the textbook menopausal picture. During perimenopause, though, levels can swing widely from month to month, so a single test can be misleading. This is why menopause is usually judged from your age, symptoms, and the pattern of your periods rather than from one blood result.
A pattern suggesting PCOS
In polycystic ovary syndrome, the baseline LH is often higher than the FSH, and tests may also show extra androgens. A panel can reveal this hormonal signature, but it cannot confirm PCOS on its own. A diagnosis also takes account of symptoms, an ultrasound of the ovaries, and checks for other causes. If androgens are raised, your doctor may look further into high testosterone in women.
When prolactin is high
A clearly raised prolactin with normal or low FSH and LH points the search toward the pituitary gland. Possible reasons range from harmless ones, such as stress or certain medicines, to a benign prolactinoma. Because prolactin can suppress the signals that drive ovulation, this pattern often explains irregular periods or trouble conceiving, and it usually deserves a repeat test and further review.
When all the hormones are low
If FSH, LH, and estradiol are all low at once, the issue may sit higher up, in the hypothalamus of the brain. This can happen with very low body weight, intense exercise, or sustained stress, a situation doctors call hypothalamic amenorrhea. Here the ovaries are capable, but the “start” signal from the brain has quietened down.
Why one abnormal number rarely means what you fear
It is easy to fixate on a single value that falls outside the range, but hormones are a moving target. FSH, LH, and estradiol change not only across the cycle but also from one cycle to the next, especially during perimenopause. A result captured on the wrong day, or during a stressful week, can look alarming and still be normal for you.
Prolactin is a good example. A needle phobia, a rushed morning, or a recent meal can nudge it upward for reasons that have nothing to do with disease. Some people also carry a harmless inactive form called macroprolactin that can inflate the reading. Doctors know this, which is why a mildly high prolactin is usually rechecked rather than acted on straight away.
Reference ranges add another layer. Two labs can report the same blood differently because they use different methods, and ranges shift with age and cycle phase. The practical takeaway is simple: a female hormone panel is most useful when a clinician reads it next to your symptoms, your history, and any earlier results. The numbers inform the conversation; they do not replace it.
When to see a doctor
A panel is a tool for a wider assessment, not a verdict. Book an appointment, and mention your results, if you notice any of the following:
- Your periods have stopped for three months or more and you are not pregnant.
- Bleeding is very heavy, very frequent, or unpredictable.
- You have been trying to conceive for 12 months without success, or 6 months if you are 35 or older.
- You have milky nipple discharge when you are not breastfeeding.
Some signs deserve prompt medical attention rather than a routine appointment. Persistent severe headaches or changes in your vision alongside a high prolactin can point to pressure from a pituitary growth and should be checked quickly. Sudden, severe pelvic pain is a separate emergency that needs its own evaluation. As always, the final interpretation of any hormone result belongs with a qualified clinician who can examine you.
Glossary
| Term | Meaning |
|---|---|
| Estradiol (E2) | The main and most active form of estrogen, made largely by growing ovarian follicles. |
| Follicle-stimulating hormone (FSH) | A pituitary hormone that tells the ovaries to grow follicles each cycle. |
| Follicular phase | The first half of the menstrual cycle, from the first day of bleeding until ovulation. |
| Hyperprolactinemia | A higher-than-normal level of prolactin in the blood. |
| Hypothalamic-pituitary-ovarian (HPO) axis | The chain of signals between the brain (hypothalamus and pituitary) and the ovaries that controls the cycle. |
| Luteal phase | The second half of the cycle, after ovulation, when progesterone rises. |
| Luteinizing hormone (LH) | A pituitary hormone whose mid-cycle surge triggers the ovary to release an egg. |
| Ovarian reserve | An estimate of the number of eggs remaining in the ovaries. |
| Prolactin | A pituitary hormone that drives milk production and can disturb periods when its level is high. |
| Reference range | The span of values a lab considers typical for a healthy group; it varies by lab, age, and cycle phase. |
Frequently asked questions
How long does it take to get female hormone panel results?
Most hormone results are ready within one to three working days, though the exact turnaround depends on your laboratory and whether the sample is sent to an outside facility. Standard markers such as FSH, LH, estradiol, and prolactin are common tests, so they are usually processed quickly. If your doctor adds less routine markers, those can take a little longer. Your clinic will tell you how the results will be shared, whether by phone, an online portal, or a follow-up visit, and it is worth asking when you should expect to hear back.
Can birth control pills affect my hormone panel results?
Yes. Combined hormonal contraception works by suppressing the body’s own FSH and LH and supplying steady hormones instead, so a panel taken while you are on the pill will not reflect your natural cycle. The same is true for the contraceptive patch, ring, implant, and hormonal coil. If the goal is to assess your underlying hormones or fertility, your doctor may ask you to time the test for after you stop, or interpret the results with the contraception in mind. Always list any hormonal method you use when you book the test.
Can a hormone panel confirm menopause, including at-home tests?
Not on its own. In someone aged 45 or older with typical symptoms and changing periods, doctors can usually recognise menopause without blood tests, because hormone levels fluctuate too much during the transition to be reliable. A high FSH with a low estradiol supports the picture but does not seal it. At-home urine kits only flag a raised FSH and cannot tell whether your ovaries are still releasing eggs, so they are best used as a prompt to discuss symptoms with your provider rather than as a definitive answer.
Does a high prolactin result mean I have a pituitary tumor?
Usually not. Many things raise prolactin temporarily, including stress, a recent meal, vigorous exercise, breast stimulation, and several common medicines. An underactive thyroid can do it too. A benign pituitary growth called a prolactinoma is only one of several possibilities, and it is more likely when the level is very high or keeps rising on repeat testing. Because of this, a single mildly raised reading is normally rechecked under calm conditions before any imaging or treatment is considered. Your doctor weighs the number against your symptoms and medicines.
Can a female hormone panel diagnose PCOS?
A panel can reveal patterns linked to polycystic ovary syndrome, such as a raised LH-to-FSH ratio or higher androgen levels, but it cannot make the diagnosis by itself. PCOS is identified using agreed criteria that combine symptoms like irregular periods or excess hair growth, signs of extra androgens on blood tests, and the appearance of the ovaries on ultrasound, after ruling out conditions that look similar. Think of the panel as one piece of evidence that helps your doctor decide whether further assessment is worthwhile.
Do I need a hormone panel if my periods are regular?
If your cycles are regular and you have no troubling symptoms, routine hormone testing is usually unnecessary, and a normal cycle is itself a reassuring sign that the system is working. Testing becomes useful when there is a specific question to answer, such as irregular or absent periods, difficulty conceiving, symptoms of perimenopause, or signs of high prolactin. Testing without a clear reason can produce borderline numbers that cause worry without changing what you would do, so it is best guided by your symptoms and your doctor.
Sources
- Follicle-Stimulating Hormone (FSH) Levels Test — MedlinePlus (U.S. National Library of Medicine)
- Follicle-Stimulating Hormone (FSH): What It Is and Function — Cleveland Clinic
- Understanding Your Menopause Diagnosis — Endocrine Society
Further reading
- FSH blood test: decoding this key hormone
- Luteinizing hormone (LH): understanding your blood results
- Estradiol: decoding this hormonal marker
- High prolactin levels: causes, symptoms, and tests
- How to read blood test results: a simple guide
Understand your lab results with AI DiagMe
Reading a female hormone panel can feel overwhelming when the report lists FSH, LH, estradiol, and prolactin next to ranges that shift with your cycle. AI DiagMe helps you make sense of these reproductive hormones in plain language, so you can walk into your next appointment understanding what your numbers describe and which questions to ask. It is built to help you understand your results, not to diagnose you or replace your doctor. Upload your report and get a clear, readable explanation in minutes.
➡️ Get your results interpreted in minutes

{kind=link}