


















A fertility blood test measures the reproductive hormones that control whether your body can release an egg, make healthy sperm, and support a pregnancy. If you have been trying to conceive, these results often arrive as a column of unfamiliar abbreviations — AMH, FSH, LH, estradiol, testosterone — that are hard to read on your own. This guide explains, in plain language, which hormones are checked for women and for men, when in the cycle each one should be drawn, and what a high or low result can suggest. Just as important, you will learn what these numbers cannot tell you, so a single value does not cause unnecessary worry. The goal is to help you walk into your next appointment understanding your own report.

What a fertility blood test actually measures
A fertility blood test is not one test. It is a small panel of hormone measurements taken from a blood sample, each giving a different clue about how the reproductive system is working. Some hormones come from the brain and signal down to the ovaries or testicles. Others are made by the ovaries or testicles themselves and signal back up. Reading them together gives a snapshot of that conversation.
It is worth setting expectations early. Blood hormones are only one part of a fertility check-up. For women, doctors also look at the ovaries and uterus with an ultrasound and check whether the fallopian tubes are open. For men, a semen analysis (a sperm count and quality test) is usually the first and most important step, because hormones alone do not show whether sperm are present or moving. According to the American Society for Reproductive Medicine, evaluation of a couple normally begins after twelve months of trying — or sooner if there are known risk factors.
So a fertility blood test answers questions like: Are the ovaries being stimulated normally? Is ovulation happening? Is the pituitary gland sending the right signals? Could a thyroid or prolactin problem be in the way? It does not, by itself, deliver a yes-or-no verdict on whether you can have a baby.
Why hormones drive fertility: the brain–gonad loop
Reproduction runs on a feedback loop between the brain and the gonads (the ovaries or testicles). A small region of the brain called the hypothalamus releases a signal to the pituitary gland. The pituitary then releases two key messenger hormones into the blood: follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
In women, FSH tells the ovaries to grow follicles (the fluid-filled sacs that hold eggs), and a mid-cycle surge of LH triggers the release of an egg. In men, FSH supports sperm production while LH tells the testicles to make testosterone. The ovaries and testicles, in turn, produce their own hormones — estrogen, progesterone, testosterone — which travel back to the brain and tell it to dial the signals up or down.
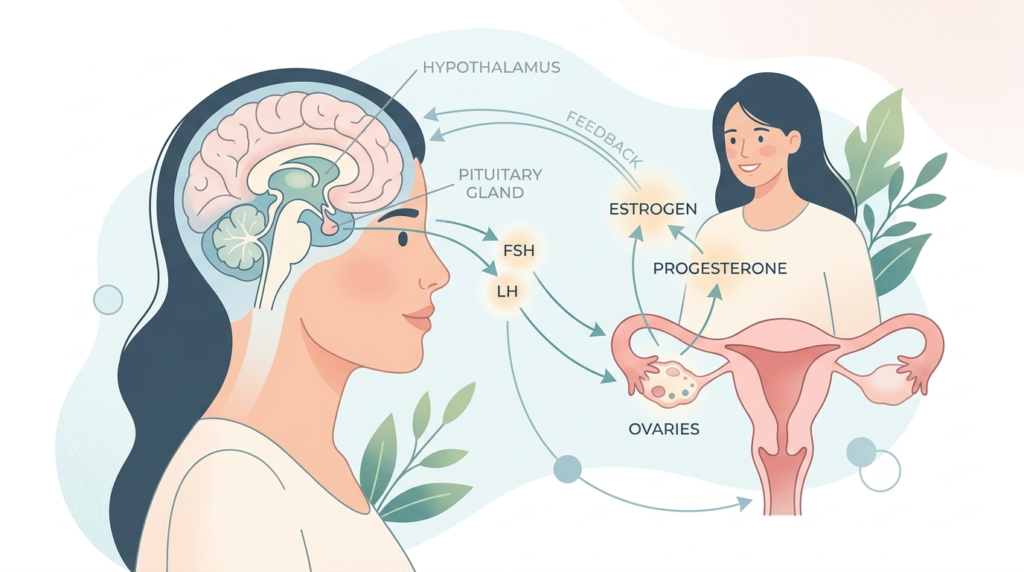
This loop is why a fertility blood test reads hormones from both ends. A high brain signal (FSH) with a weak ovary response, for example, points to a different problem than a low brain signal with healthy ovaries. The pattern matters more than any single number.
Female fertility blood test: hormones to check
For women, a fertility blood test focuses on two questions: how many eggs are left (ovarian reserve) and is ovulation actually happening. Different hormones answer each, and several must be drawn on specific days of the cycle.
Day 2–5 hormones: FSH, LH and estradiol
Early in the cycle — most often on day three, counting the first day of your period as day one — the ovaries are quiet, which makes this the cleanest moment to measure baseline signals. A blood draw at this point typically checks follicle-stimulating hormone (FSH), luteinizing hormone (LH) and estradiol, the main form of estrogen.
A clearly raised FSH on day three, especially alongside a low estradiol, can suggest the ovaries are working harder to recruit eggs — a sign that may point toward diminished ovarian reserve. The LH-to-FSH ratio and the pattern of these three together also help doctors distinguish conditions such as polycystic ovary syndrome from other causes of irregular cycles.
AMH: the ovarian reserve marker you can test any day
Anti-Müllerian hormone (AMH) is produced by small follicles in the ovaries, so its level reflects roughly how many eggs remain. Unlike FSH, AMH stays fairly stable across the cycle, so it can be drawn on almost any day — a practical advantage. AMH tends to fall with age.
Here is the crucial caveat. As the U.S. National Library of Medicine explains, an AMH test can estimate the size of your ovarian reserve, but it cannot tell you about the health of your eggs and cannot predict whether you will get pregnant. A low AMH does not mean pregnancy is impossible, and a high AMH is not a guarantee. It is one input, not a forecast.
Progesterone: confirming that ovulation happened
Progesterone rises in the second half of the cycle, after an egg is released. A blood test taken in the mid-luteal phase — roughly seven days before your next expected period, often called the “day 21” test in a 28-day cycle — checks whether progesterone has climbed. A clear rise is good evidence that ovulation occurred that month. A flat result may simply mean the test was mistimed in an irregular cycle, which is why doctors sometimes repeat it.
Prolactin and thyroid: the upstream disruptors
Two hormones from outside the ovaries can quietly stop ovulation. Prolactin, the hormone behind breast milk, can suppress the cycle when it is too high. And the thyroid, checked through thyroid-stimulating hormone (TSH), influences both ovulation and early pregnancy. Because both are easy to test and often treatable, they are usually part of the female panel. When excess male-type hormones are suspected — for example in polycystic ovary syndrome — doctors may add testosterone and sex hormone-binding globulin (SHBG), a protein that controls how much testosterone is active. The full set is often ordered together as a female hormone panel.
Male fertility blood test: hormones to check
Male fertility evaluation starts with a semen analysis, not a blood test, because the most common male issue is a problem with the number, shape, or movement of sperm — which hormones cannot reveal. Blood hormones become useful when the semen analysis is abnormal, when sperm are very low or absent, or when there are symptoms of low testosterone such as low sex drive or fatigue.
Testosterone and SHBG
Testosterone is the main hormone behind sperm production, libido and muscle and bone strength. Labs often report both total testosterone and free testosterone (the active portion), and may add SHBG to interpret them, since SHBG decides how much testosterone is available to the body. Testosterone naturally peaks in the morning, so the sample is usually taken between 8 and 10 a.m. for an accurate reading.
FSH and LH in men
FSH and LH tell doctors where a testosterone problem comes from. Low testosterone paired with high FSH and LH points to the testicles themselves, because the brain is shouting but the testicles are not responding. Low testosterone with low or normal FSH and LH points instead toward the pituitary or hypothalamus in the brain. These markers are commonly grouped into a male hormone panel.
Prolactin and thyroid
As in women, a high prolactin level or an out-of-range thyroid can lower testosterone and reduce sperm production. So prolactin and TSH are often added when the picture is unclear, especially if testosterone is unexpectedly low.
The fertility hormone panel at a glance
The table below summarizes the hormones most often included in a fertility blood test, who they apply to, the best time to measure them, and what an abnormal result may suggest. Reference ranges differ between laboratories, so use this as a map of what each marker means, not as a set of target numbers.
| Hormone | Mainly checked in | Best timing | What an abnormal result may suggest |
|---|---|---|---|
| FSH | Women and men | Women: day 2–5; men: any day | High in women may signal low ovarian reserve; high in men points to a testicular issue |
| LH | Women and men | Women: day 2–5 (and mid-cycle for the surge); men: any day | Helps locate the source of a hormone problem; LH:FSH pattern aids PCOS assessment |
| Estradiol (E2) | Women (small role in men) | Women: day 2–5 | Interpreted with FSH to judge ovarian function |
| AMH | Women | Any day | Lower with age; estimates egg quantity, not egg quality or your chance of pregnancy |
| Progesterone | Women | Mid-luteal (about day 21) | A clear rise confirms ovulation happened that cycle |
| Testosterone (total and free) | Men (and women if PCOS suspected) | Men: morning (8–10 a.m.) | Low in men can affect sperm and libido; high in women may indicate PCOS |
| SHBG | Men and women | With testosterone | Changes how much testosterone is active; helps interpret testosterone levels |
| Prolactin | Women and men | Any day | High levels can suppress ovulation or lower testosterone |
| TSH (thyroid) | Women and men | Any day | Thyroid imbalance can disrupt ovulation, cycles and sperm production |
Timing matters: when in your cycle to test
For women, when a fertility blood test is drawn changes the result, so timing is not a detail — it is part of the test. The two anchor points to remember are early-cycle and mid-luteal.
- Day 2–5 (early cycle): FSH, LH and estradiol, to read the baseline ovarian signals.
- AMH and TSH/prolactin: any day, since they do not swing with the cycle.
- Mid-luteal, about day 21 of a 28-day cycle: progesterone, to confirm ovulation roughly a week before your period is due.
If your cycles are longer or shorter than 28 days, the “day 21” progesterone test shifts accordingly — it should land about seven days before your expected period, not on the calendar’s 21st. Tracking ovulation at home, for example with an ovulation test that detects the LH surge, can help you and your clinician choose the right day. For men, the main timing rule is simpler: draw testosterone in the morning, when it is highest.
What your results can — and can’t — tell you
This is the section most worth reading twice. A fertility blood test gives clues, not conclusions, and several limits are important to understand before you interpret your own report.
First, a single out-of-range value is rarely a diagnosis. Hormones move with the cycle, the time of day, stress, illness and recent travel, so doctors often repeat an abnormal test rather than act on one reading. Second, reference ranges vary between laboratories and depend on your age, sex and cycle day; a number flagged “high” on one report might sit inside the normal range on another. If you want a general primer on interpreting lab values, see our guide on how to read blood test results.
Third — and this is where many people are misled — ovarian reserve markers like AMH and FSH measure egg quantity, not egg quality, and they do not predict whether you will conceive naturally. The American Society for Reproductive Medicine is explicit that ovarian reserve tests should not be used to predict the chance of spontaneous pregnancy or to deny anyone fertility care. The final interpretation belongs to a doctor who can read your hormones alongside your history, your ultrasound and, for men, the semen analysis.
When to see a doctor
You do not need to figure out fertility testing alone, and there are clear points at which professional evaluation is recommended rather than optional.
- You have been having regular, unprotected sex for 12 months without conceiving.
- You are a woman over 35 and have been trying for 6 months, or you are over 40 — both warrant earlier evaluation.
- Your periods are irregular, very heavy, very painful, or absent.
- You have a known condition that can affect fertility, such as polycystic ovary syndrome, endometriosis, a thyroid disorder, or a history of pelvic infection or cancer treatment.
- A man has symptoms of low testosterone, a known testicular problem, or an abnormal semen analysis.
Seeing a doctor sooner does not mean something is wrong; it means any treatable cause can be found while there is the most time to act. Your clinician will also order the right tests in the right sequence, so you are not paying for or worrying about results you do not yet need. If you are wondering about turnaround, our article on how long blood test results take explains typical waiting times.
Glossary
- AMH (anti-Müllerian hormone): A hormone made by small ovarian follicles that reflects how many eggs remain. It estimates egg quantity, not egg quality.
- Estradiol (E2): The main form of estrogen, produced mostly by the ovaries. Read together with FSH to judge ovarian function.
- FSH (follicle-stimulating hormone): A pituitary hormone that tells the ovaries to grow follicles and supports sperm production in men.
- LH (luteinizing hormone): A pituitary hormone whose mid-cycle surge triggers ovulation; in men it drives testosterone production.
- Ovarian reserve: A measure of the number of eggs remaining in the ovaries, which naturally declines with age.
- Progesterone: A hormone that rises after ovulation and prepares the uterine lining for pregnancy; a mid-luteal rise confirms ovulation.
- Prolactin: The hormone behind breast milk; when too high it can stop ovulation in women and lower testosterone in men.
- Semen analysis: A laboratory test of sperm number, shape and movement — the first-line test for male fertility.
- SHBG (sex hormone-binding globulin): A protein that binds testosterone and estrogen and controls how much is active in the body.
- TSH (thyroid-stimulating hormone): A pituitary hormone used to check thyroid function, which influences ovulation and sperm production.
Frequently asked questions
How much does a fertility blood test cost, and is it covered by insurance?
Costs vary widely depending on how many hormones are tested and whether the blood is drawn through a clinic, a hospital, or a direct-to-consumer service. Insurance coverage also varies. Some plans cover fertility evaluation when a doctor considers it medically necessary, while others exclude fertility testing or cover only part of it; in some regions coverage is shaped by local mandates. The most reliable approach is to ask your provider which hormones they recommend and then check directly with your insurer about what is covered before testing, so there are no surprises.
Are at-home fertility hormone tests accurate?
At-home kits can measure hormones such as AMH or FSH from a finger-prick sample, and a good one can give a reasonable estimate of ovarian reserve. Their main limits are timing and context. Cycle-dependent hormones must be collected on the correct day to mean anything, and a result has little value without the rest of the picture — your history, an ultrasound, and a clinician’s interpretation. At-home tests can be a useful starting point, but an abnormal or worrying result should always be discussed with a doctor rather than acted on alone.
Do I need to fast before a fertility blood test?
Most reproductive hormones — FSH, LH, estradiol, progesterone, AMH, testosterone and prolactin — do not require fasting. The more important preparations are timing and a few sample-handling rules: drawing cycle-dependent hormones on the right day, measuring testosterone in the morning, and, with some labs, pausing high-dose biotin supplements for a couple of days, since biotin can interfere with certain hormone assays. Always follow the specific instructions on your lab request, as protocols differ between laboratories.
Does age change what a fertility blood test shows?
Yes, particularly for women. Ovarian reserve falls with age, so AMH tends to decline and day-3 FSH tends to rise over time. This is a normal, expected pattern rather than a disease. It is also why evaluation is recommended sooner for women over 35 and without delay over 40 — not because testing changes, but because acting early leaves the most options open. In men, testosterone declines more gradually with age, and any sharp drop is usually investigated for a specific cause.
What if my periods are irregular — when should I test?
Irregular cycles make timed tests trickier, because the usual “day 3” and “day 21” landmarks are harder to pin down. Hormones that do not depend on cycle day — AMH, TSH and prolactin — can still be drawn anytime and are often especially informative when periods are unpredictable. For ovulation-related tests like progesterone, a clinician may use ovulation tracking to choose the day, or repeat the test across cycles. Irregular periods are themselves a reason to seek evaluation, since they can point to a treatable cause.
How long do fertility blood test results take?
Common reproductive hormones are widely run, and many results come back within a few days, though turnaround depends on the laboratory and the specific markers ordered. Some specialized assays take longer because they are processed in batches or sent to a reference lab. If you have not heard back within the timeframe your clinic mentioned, it is reasonable to follow up. You can read more about typical waiting times in our guide on how long blood test results take.
Sources
- Female infertility: diagnosis and treatment — Mayo Clinic
- Fertility evaluation of infertile women: a committee opinion (2021) — American Society for Reproductive Medicine
- Anti-Müllerian Hormone Test — MedlinePlus (U.S. National Library of Medicine)
Further reading
- Female hormone panel: what your results mean
- Male hormone panel: what it measures
- Blood tests during pregnancy: what’s checked
- How to read blood test results
- Pregnancy test guide: accuracy and interpretation
Understand your lab results with AI DiagMe
A fertility blood test often comes back as a column of numbers — AMH, FSH, LH, estradiol, testosterone, prolactin and thyroid (TSH) — with reference ranges that shift by sex and cycle day. AI DiagMe reads your reproductive hormone results alongside the rest of your panel and explains, in plain language, what each value means and which ones may be worth raising with your doctor. It is a tool to help you understand your results, not a diagnosis, and it does not replace your physician. If you have a recent fertility blood test in hand, see what your numbers are telling you.
➡️ Get your results interpreted in minutes
{kind=link}