


















A kidney function panel is a group of blood tests that shows how well your kidneys are filtering waste and keeping your body’s chemistry in balance. If you have just received your results and you are trying to make sense of values like creatinine, eGFR, and BUN, this guide is for you.
Your kidneys quietly clean your blood every minute of the day. When that filtering slows down, a few specific values shift before you ever feel a symptom — which is exactly why this panel exists.
This article explains, in plain language, what each test on a kidney function panel measures, what the normal ranges look like, and how to read your results as a pattern rather than a single worrying number. You will also see how this panel compares to a metabolic panel, the one urine test that completes the picture, and the warning signs worth a conversation with your doctor.
What is a kidney function panel?
A kidney function panel is a blood test that measures several substances at once to estimate how well your kidneys are working. You may also see it written as a renal panel or renal function panel — “renal” simply means “relating to the kidneys,” so all three names point to the same idea.
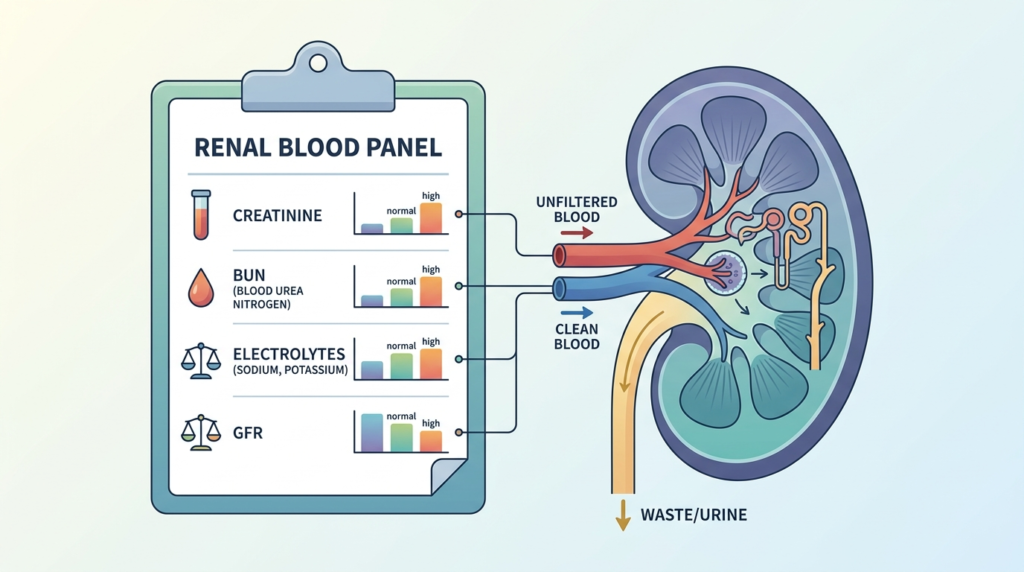
The test works by checking the waste products your kidneys are supposed to remove, plus the minerals they help keep in balance. When the kidneys filter normally, these values stay inside expected ranges. When filtering slows, waste builds up and the balance shifts.
Doctors order a kidney function panel for several reasons: as a routine check-up, to screen people at higher risk, to monitor a known kidney condition over time, or to make sure a medication is safe for the kidneys. It is one of the most common blood tests because the kidneys touch almost every system in the body.
It helps to know what the kidneys actually do. These two fist-sized organs filter your entire blood supply many times a day, clearing waste, balancing salts and water, and helping control blood pressure. The panel was built around the handful of substances that shift first when this filtering falters, which is why a single blood draw can reveal so much about an organ you never feel working.
What tests are in a kidney function panel?
The exact list varies slightly from one lab to another, but most kidney function panels group their measurements into a few familiar categories. Below is what you are most likely to see on your report.
Waste products your kidneys clear
These markers rise when the kidneys are not removing waste efficiently.
- Creatinine is a waste product made during normal muscle activity. The kidneys filter it out steadily, so a higher level can signal that filtering has slowed. You can read more in our guide to creatinine as a kidney marker.
- eGFR (estimated glomerular filtration rate) is a calculation, not a direct measurement. It uses your creatinine result along with your age and sex to estimate how much blood your kidneys filter each minute. It is the headline number for kidney health — see our explainer on what eGFR means.
- BUN (blood urea nitrogen) measures urea, a waste product left over when your body breaks down protein. Our BUN test guide covers what high and low values can mean.
- Uric acid is another waste product the kidneys clear. High levels are linked to gout and, in some cases, to reduced filtering, so it sometimes appears on a kidney-focused panel.
Electrolytes and minerals
Electrolytes are minerals that carry a small electrical charge and help your nerves, muscles, and fluid balance work properly. Healthy kidneys keep them within a narrow window. A panel often reports sodium, potassium (a mineral that strongly affects the heart and muscles, covered in our potassium test guide), chloride, and bicarbonate. It may also include the minerals calcium and phosphorus, which the kidneys help regulate.
Other values you may see
Some panels add albumin, a protein made by the liver, and glucose (blood sugar). These are not pure kidney markers, but they give useful context — for example, very low albumin or poorly controlled blood sugar can both affect kidney health over time.
Kidney function panel normal ranges, and what high or low means
Reference ranges are guideposts, not verdicts. They vary by laboratory, and what counts as “normal” can shift with your age, sex, and muscle mass. Your report will print the specific range your lab uses, usually in a column next to your result. The table below gives the approximate adult ranges for the main kidney markers.
| Marker | Typical adult range* | What an out-of-range value can suggest |
|---|---|---|
| Creatinine | ~0.7–1.3 mg/dL (men), ~0.6–1.1 mg/dL (women) | Higher: slower filtering, dehydration, high muscle mass. Lower: low muscle mass |
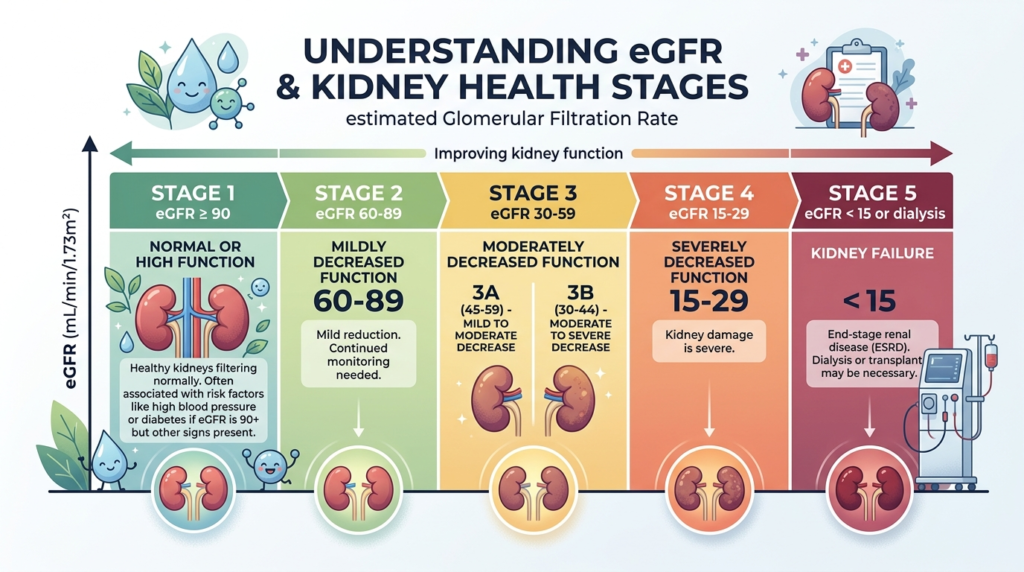
| eGFR | 90+ (ideal); 60–89 mildly reduced; under 60 for 3+ months may indicate kidney disease | A falling eGFR over time is the key warning sign |
| BUN (urea nitrogen) | ~7–20 mg/dL | Higher: dehydration, high-protein diet, reduced filtering. Lower: low protein intake, liver issues |
| BUN-to-creatinine ratio | roughly 10:1 to 20:1 | A high ratio often points to dehydration; both rising together points more to the kidney itself |
| Uric acid | ~3.5–7.2 mg/dL (men), ~2.6–6.0 mg/dL (women) | Higher: gout, reduced clearance, certain diets |
*Approximate values for general guidance only; always use the reference range printed on your own report.
For the electrolytes and minerals, the usual adult ranges are roughly: sodium 135–145 mmol/L, potassium 3.5–5.0 mmol/L, chloride 96–106 mmol/L, bicarbonate 22–29 mmol/L, calcium 8.5–10.2 mg/dL, and phosphorus 2.5–4.5 mg/dL. Small drifts outside these windows are common and often harmless; larger or repeated shifts are what prompt a closer look.
How to read your kidney function panel results
The single most useful habit is this: read your panel as a pattern, not as one number in isolation. A laboratory result is a snapshot, and many everyday factors can nudge a value up or down without meaning anything is wrong.
Start with the eGFR, because it is the best overall summary of filtering. An eGFR of 90 or above is generally healthy, while a value under 60 that stays low across more than one test is the finding doctors take most seriously. eGFR also drops gently with age and can dip temporarily when you are dehydrated, so a one-off low reading is not the same as a diagnosis.
Next, look at creatinine and BUN together. The relationship between them is genuinely informative. When the BUN-to-creatinine ratio is high but creatinine itself is fairly normal, the cause is often outside the kidney — most commonly dehydration or reduced blood flow. When creatinine and BUN rise side by side, attention turns to the kidney’s own filtering. Our guides on the BUN/creatinine ratio and on high BUN and creatinine together walk through these patterns.
Finally, remember what can skew a result. A high-protein meal, intense exercise, dehydration, and some medicines (including common anti-inflammatory painkillers) can all change these numbers for a day or two. That is why doctors compare results over time. A trend — three readings drifting in the same direction — tells a clearer story than any one value, and the final interpretation always belongs to a clinician who knows your full history.
Kidney function panel vs. metabolic panel: what is the difference?
This is one of the most common points of confusion, and the short answer is reassuring: there is a lot of overlap. A basic metabolic panel (BMP) and a comprehensive metabolic panel (CMP) both already contain the core kidney markers, so a metabolic panel does check kidney function. A dedicated kidney function panel simply puts the renal markers front and centre.
| Test | Main focus | Kidney markers included | Also includes |
|---|---|---|---|
| Kidney (renal) function panel | The kidneys | Creatinine, eGFR, BUN, electrolytes | Sometimes calcium, phosphorus, albumin |
| Basic metabolic panel (BMP) | Chemistry and kidney basics | Creatinine, BUN, electrolytes | Glucose, calcium |
| Comprehensive metabolic panel (CMP) | Chemistry, kidney and liver | Creatinine, BUN, electrolytes | Glucose, calcium, albumin, liver tests |
In practice, if your doctor has run a CMP, your kidney function has already been screened. The difference is that the CMP adds liver enzymes and a few extra proteins. A separate kidney panel becomes useful when the focus is specifically on the kidneys — for monitoring, for example. If you also want to understand how blood-count tests fit alongside chemistry tests, our comparison of CBC vs CMP is a helpful companion read.
One myth is worth clearing up: a lipid panel measures cholesterol and triglycerides, not kidney function. The two tests are sometimes drawn from the same blood sample, but a lipid result tells you nothing direct about how your kidneys are filtering.
The urine test that completes the picture
A blood-based kidney function panel is powerful, but on its own it can miss the earliest stage of kidney damage. That is because the kidneys can start leaking small amounts of protein into the urine long before the eGFR falls. To catch this, the kidney health you read in blood is paired with a simple urine test.
That test is the urine albumin-to-creatinine ratio (uACR). It measures albumin — a protein that should stay in the blood — appearing in the urine, a sign sometimes called albuminuria or proteinuria (protein in the urine). A small leak is one of the first warning signals, and our guide to microalbuminuria explains why it matters so early.
The uACR is read in milligrams of albumin per gram of creatinine: under 30 mg/g is normal, 30 to 300 mg/g is moderately increased, and above 300 mg/g is severely increased. You can learn how this ratio is calculated in our explainer on the albumin/creatinine ratio.
Major kidney-health bodies recommend a two-test approach: an eGFR from blood plus a uACR from urine. Together they give a far more complete view than either marker alone. A normal blood panel paired with a raised uACR, for example, can be the very first hint that something needs watching — often long before the eGFR moves.
When to get tested, and when to see a doctor
Kidney disease is often silent in its early stages, so testing — not symptoms — is usually how problems are found first. You are more likely to be offered a kidney function panel if you have certain risk factors, and you should be the most proactive about regular checks if any apply to you.
Common reasons for routine kidney testing include living with diabetes or high blood pressure — the two leading causes of kidney disease — as well as heart disease, a family history of kidney failure, older age, or taking medications that can affect the kidneys. For many people with diabetes or high blood pressure, an annual kidney check is advised.
Most standalone kidney panels do not require fasting. If your panel is bundled with a glucose or cholesterol test, however, the lab may ask you to fast beforehand, so it is always worth checking the instructions on your appointment.
The test itself is straightforward. It is a standard blood draw from a vein in your arm, usually taking only a minute or two, and most laboratories return results within a day or two. No special recovery is needed, and you can return to your normal routine straight afterwards.
Some symptoms deserve a prompt conversation with a healthcare professional, especially if they are new or persistent:
- Swelling in the legs, ankles, feet, or around the eyes
- Foamy or bubbly urine, or a noticeable change in how often you urinate
- Persistent tiredness, poor appetite, or nausea
- Blood in the urine
- Sudden, severe pain in the back or side, which can signal kidney stones and may need urgent care
Above all, keep one principle in mind: a single abnormal value is not a diagnosis. Doctors weigh your full panel, your symptoms, your history, and how your numbers change over time before drawing any conclusion. Your results are the start of a conversation, not the end of one.
Glossary
- Albumin: A protein made by the liver that normally stays in the blood. Finding it in the urine can be an early sign of kidney damage.
- BUN (blood urea nitrogen): A measure of urea, a waste product made when the body breaks down protein. It rises when the kidneys filter less, but also with dehydration.
- Chronic kidney disease (CKD): A long-term reduction in how well the kidneys filter, generally defined as filtering below normal for more than three months.
- Creatinine: A waste product from normal muscle activity that the kidneys clear from the blood. Higher levels can point to slower filtering.
- eGFR (estimated glomerular filtration rate): A calculated estimate of how much blood the kidneys filter each minute, based on creatinine, age, and sex.
- Electrolytes: Minerals such as sodium and potassium that carry an electrical charge and help control fluid balance, nerves, and muscles.
- Metabolic panel (BMP/CMP): A broader blood test of body chemistry that already includes the main kidney markers; the comprehensive version (CMP) also covers the liver.
- Renal: A medical word meaning “relating to the kidneys.”
- uACR (urine albumin-to-creatinine ratio): A urine test that detects small amounts of protein (albumin) leaking from the kidneys, often the earliest warning sign.
Frequently asked questions
Do I need to fast before a kidney function panel?
For most people, no. A standalone kidney or renal function panel does not usually require fasting, because the kidney markers themselves are not strongly affected by a recent meal. The exception is when the test is combined with others. If your blood draw also includes a fasting glucose or a cholesterol (lipid) test, the laboratory may ask you to avoid food and drink for several hours beforehand. Because the rules depend on the exact tests ordered, the safest approach is to follow the written instructions from your clinic or to call and ask. When in doubt, drinking water is generally fine and even encouraged, since being well hydrated can give more reliable results.
Does a comprehensive metabolic panel check kidney function?
Yes. A comprehensive metabolic panel (CMP) includes creatinine, BUN, and the main electrolytes, which are the core measurements used to judge kidney function. A basic metabolic panel (BMP) does the same with a slightly shorter list. So if your doctor has already ordered a CMP, your kidneys have been screened as part of it. A separate kidney function panel is mainly useful when the focus is specifically on the kidneys, such as monitoring a known condition. In many cases, the difference between the two is more about emphasis and labelling than about which kidney markers are measured.
Can a lipid panel show how my kidneys are working?
No. A lipid panel measures fats in the blood, mainly total cholesterol, LDL, HDL, and triglycerides. It is used to assess heart and blood-vessel risk, not kidney filtering. The confusion often arises because a lipid panel and a kidney panel can be drawn from the same blood sample during one visit. They are still separate tests with separate purposes, and a lipid result will not tell you anything direct about creatinine, eGFR, or how well your kidneys clear waste. To assess kidney function, you need the kidney-specific markers or a metabolic panel that contains them.
Should I worry if just one value on my panel is abnormal?
A single value slightly outside the reference range is common and rarely a cause for alarm on its own. Many everyday factors can shift a result for a day or two, including dehydration, a high-protein meal, intense exercise, and certain medications. This is why clinicians look at the whole panel together and, where needed, repeat the test to see whether the change is real and lasting. A trend across several results carries far more weight than one snapshot. If a value is markedly abnormal or keeps moving in the same direction, your doctor will investigate further rather than relying on a single reading.
Is a kidney function panel the same as a urine test?
Not quite — they are partners. A kidney function panel is a blood test that measures waste products and electrolytes such as creatinine, eGFR, and BUN. A urine test, such as the urine albumin-to-creatinine ratio (uACR), checks for protein leaking into the urine. Each catches something the other can miss: blood markers show how much filtering capacity remains, while the urine test can reveal very early damage before blood values change. For a complete picture of kidney health, the two are often used side by side, which is why your doctor may order both at the same time.
Can children and older adults use the same reference ranges?
Reference ranges are not one-size-fits-all. eGFR naturally declines with age, so a value that is expected in an older adult might be flagged differently in a younger person. The eGFR calculation is also considered less precise in children, during pregnancy, and in people with unusually high muscle mass, because those situations affect creatinine in ways the equation does not fully capture. Children typically have age-specific ranges calculated with a method designed for them. For these reasons, results should always be interpreted by a clinician in light of the person’s age, sex, and overall health rather than compared to a single universal cut-off.
Sources
- Testing for Chronic Kidney Disease — Centers for Disease Control and Prevention (CDC)
- Kidney Function Tests: Types, Results & Follow Up — Cleveland Clinic
- Know Your Kidney Numbers: Two Simple Tests — National Kidney Foundation
Further reading
- Creatinine: Understanding this blood marker for kidney function
- Estimated Glomerular Filtration Rate (eGFR) explained
- BUN (Urea): Understanding your test results
- BUN/Creatinine Ratio: meaning and levels
- ACR (Albumin/Creatinine Ratio): decoding this renal marker
Understand your lab results with AI DiagMe
Reading a kidney function panel can feel overwhelming when waste markers, electrolytes, and an eGFR all land on the same page. AI DiagMe helps you make sense of tests like creatinine, your eGFR (kidney filtration rate), BUN, and the urine albumin-to-creatinine ratio, turning raw numbers into clear, plain-language context. It is designed to help you understand your results and prepare better questions for your appointment — it supports your doctor’s role, it does not replace it. When your next set of results arrives, you do not have to decode them alone.
➡️ Get your results interpreted in minutes
{kind=link}