

















An MCV blood test measures the average size of your red blood cells and is one of the most common values reported on a complete blood count. If your report shows an MCV result flagged high or low, it is a useful clue rather than a diagnosis on its own. In this article you’ll learn what the MCV blood test measures, why red blood cell size matters, how to read your number against the normal range, and what high or low results can point to, with links to deeper guides if your value falls outside the typical range.
What does an MCV blood test measure?
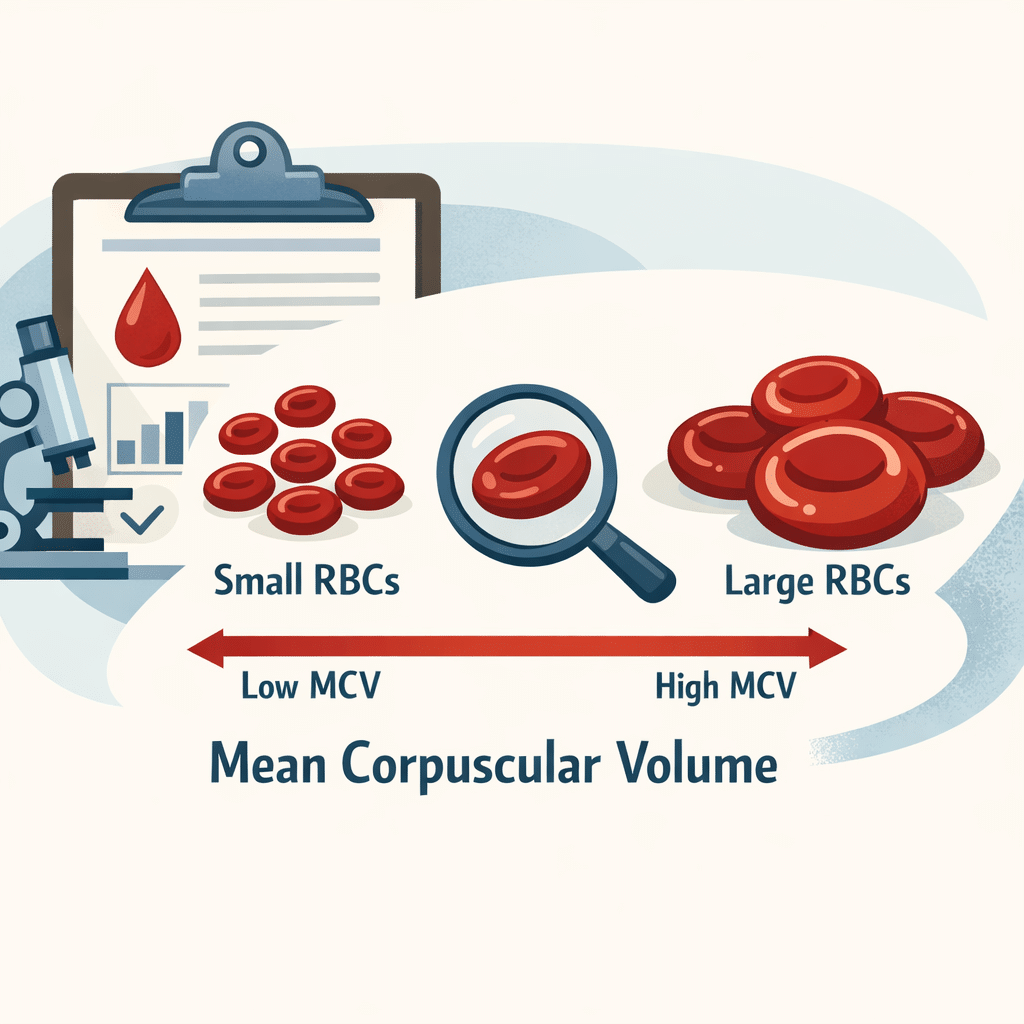
MCV stands for mean corpuscular volume, the average volume of a single red blood cell, expressed in femtoliters (fL), an extremely small unit of volume. Red blood cells, also called erythrocytes, are made in your bone marrow and carry oxygen from your lungs to every tissue in your body, then carry carbon dioxide back to be exhaled.
The size of these cells affects how efficiently they do that job. An MCV blood test tells your doctor whether your red blood cells are a typical size, smaller than expected (a pattern called microcytosis), or larger than expected (macrocytosis). Because cell size often reflects what is happening inside the cell, MCV gives an early hint about nutritional status, bone marrow function, and certain inherited conditions.
Why the MCV blood test matters
The MCV blood test is not ordered on its own. It is one of several red blood cell indices reported automatically as part of a complete blood count, alongside mean corpuscular hemoglobin (MCH) and mean corpuscular hemoglobin concentration (MCHC). Together, these values help your doctor narrow down the cause of anemia or other red blood cell problems, often before you have any symptoms.
A window into nutritional status
MCV often mirrors your body’s reserves of iron, vitamin B12, and folate (vitamin B9). A low MCV frequently signals iron deficiency, since insufficient iron limits hemoglobin production and shrinks red blood cells. A high MCV, by contrast, often points to a shortage of vitamin B12 or folate, both of which are needed for normal DNA synthesis during red blood cell formation.
A clue to conditions beyond diet
An abnormal MCV can also reflect inherited conditions such as thalassemia, chronic liver disease, low thyroid function, certain medications, or, less commonly, bone marrow disorders. Because the list of possible causes is broad, doctors interpret MCV alongside your symptoms, other blood counts, and sometimes a blood smear examined under a microscope.
How results guide next steps
An out-of-range MCV blood test result often determines what your doctor orders next. A low MCV typically prompts iron studies, while a high MCV usually leads to vitamin B12 and folate testing, and sometimes liver or thyroid function tests. MCV can also help track how well a treatment, such as iron or B12 supplementation, is working over time.
Normal MCV range and how to read your result
On a lab report, MCV usually appears in the hematology or complete blood count section. For most adults, the standard reference range for the MCV blood test is about 80 to 100 fL. Values below roughly 80 fL are generally classified as low (microcytic), and values above roughly 100 fL as high (macrocytic).
Reference ranges are not perfectly universal. Each laboratory sets its own range based on the equipment it uses and the population it serves, so you may see minor variations between labs. Always compare your result to the range printed on your own report rather than to a number found online. Look for symbols such as an upward arrow (high) or downward arrow (low), or an asterisk marking an atypical value; some labs use multiple asterisks to show how far a result sits from the expected range.
High MCV vs. low MCV: a quick comparison
The table below summarizes how the two directions typically differ. It is a starting point for understanding your report, not a substitute for your doctor’s interpretation.
| Característica | Low MCV (microcytosis) | High MCV (macrocytosis) |
|---|---|---|
| Typical threshold | Below about 80 fL | Above about 100 fL |
| Most common cause | Deficiencia de hierro | Deficiencia de vitamina B12 o folato |
| Other possible causes | Thalassemia, chronic inflammation, sideroblastic anemia, lead exposure | Chronic alcohol use, liver disease, hypothyroidism, some medications, myelodysplastic syndrome |
| Typical follow-up tests | Iron studies, ferritin, reticulocyte count | Vitamin B12 and folate levels, liver and thyroid tests |
For a deeper dive into either direction, including symptoms, treatment options, and what to expect from follow-up care, see our dedicated guides to low MCV causes, symptoms, and treatments y understanding high MCV levels and their causes.
Can MCV be normal and still signal a problem?
Yes. It is possible to have anemia with a completely normal MCV, sometimes called normocytic anemia. This pattern can occur with sudden blood loss, kidney failure, or a combination of deficiencies that cancel each other out, such as concurrent iron and vitamin B12 deficiency. This is one reason MCV is always read alongside hemoglobin, hematocrit, and your red blood cell count rather than in isolation. Our guide to reading a complete blood count walks through how all of these values fit together.
When to see a doctor about your MCV blood test
Most mildly abnormal MCV results are not emergencies and simply prompt further testing or a repeat blood draw. Still, some situations deserve prompter attention.
Consider contacting a healthcare provider sooner if you notice:
Persistent fatigue, weakness, or shortness of breath with activity, which can accompany anemia regardless of cell size. Pale skin, brittle nails, or unusual cravings for non-food items such as ice, which can suggest iron deficiency. Numbness, tingling, balance problems, or memory changes, which can occur with vitamin B12 deficiency affecting the nervous system. A markedly abnormal MCV, especially alongside low hemoglobin, or any result your doctor has specifically flagged for follow-up. Chest pain, fainting, or a rapid heartbeat, which warrant urgent evaluation rather than waiting for a scheduled appointment.
A single mildly out-of-range MCV blood test result, with no symptoms, is often simply rechecked at a later date rather than treated immediately.
How doctors investigate an abnormal MCV blood test
When your MCV falls outside the reference range, your doctor typically looks at the broader pattern before ordering more tests. They will check whether hemoglobin and hematocrit are also low, since MCV combined with these values helps classify the type of anemia present. A reticulocyte count, which measures how many new red blood cells your bone marrow is producing, can show whether your body is responding appropriately to a deficiency.
For a low MCV, iron studies, including ferritin, serum iron, and total iron-binding capacity, are the usual next step; our iron studies panel guide explains how these markers fit together. For a high MCV, vitamin B12 and folate levels are typically checked first, alongside liver and thyroid function; you can learn more in our guides to the análisis de sangre de ácido fólico and to interpreting elevated vitamin B12 results. In some cases, doctors also examine a blood smear under a microscope or order hemoglobin electrophoresis to rule out thalassemia.
Diet and lifestyle factors that influence MCV
Because MCV often reflects nutrient status, diet plays a meaningful role in prevention and recovery once a cause is identified. If a low MCV traces back to iron deficiency, iron-rich foods such as red meat, poultry, legumes, and dark leafy greens can help, especially when paired with a vitamin C source like citrus fruit, which improves iron absorption. Tea and coffee taken with meals can reduce iron uptake, so spacing them apart from iron-rich meals is a simple, practical habit.
If a high MCV relates to vitamin B12 or folate deficiency, prioritizing dairy, eggs, fish, and fortified cereals for B12, plus leafy greens and legumes for folate, supports recovery. Limiting alcohol intake matters too, since chronic alcohol use is a common, often overlooked, cause of macrocytosis independent of any vitamin deficiency. These dietary steps support treatment; they do not replace it, and any suspected deficiency should still be confirmed and monitored by a clinician.
How the MCV blood test is performed
The MCV blood test requires nothing more than a standard blood draw. A healthcare professional collects a small blood sample from a vein in your arm, and the value is calculated automatically by the same analyzer that processes your complete blood count. No fasting or special preparation is needed unless the same blood draw includes other tests, such as a fasting glucose or lipid panel, that do require it. Results are typically available within hours to a couple of days, depending on the laboratory.
Avances científicos recientes
Recent research has focused on making better use of the MCV blood test and related red blood cell indices, particularly by combining them with computer-based pattern recognition to speed up diagnosis.
A 2025 study analyzed complete blood count data, including MCV, to build a computer model that could help tell apart iron deficiency anemia from aplastic anemia, a rarer and more serious bone marrow condition, using routine blood values already collected during standard testing. What this means for you: MCV and related red blood cell measurements may increasingly support faster, more consistent distinctions between common and rare causes of anemia, potentially shortening the path from an abnormal blood count to the right follow-up test. This research is still preliminary and based on a single hospital dataset, so it has not yet changed everyday clinical practice, but it points toward MCV becoming an even more useful early signal over time.
A related 2024 study built and tested a computer model using MCV, along with mean corpuscular hemoglobin (MCH) and red cell distribution width (a measure of how much red blood cell size varies), to distinguish iron deficiency anemia from thalassemia trait, a genetic condition that can look similar on a basic blood count. What this means for you: telling these two conditions apart matters practically, because thalassemia trait does not respond to iron supplements and unnecessary iron can build up harmfully over time, while true iron deficiency does need iron replacement. The model performed well in the study population, but it was developed and tested at specific hospitals, so its accuracy in other populations and laboratories is still being confirmed. For now, these approaches are research tools rather than something your local lab uses directly, but they illustrate how the humble MCV blood test continues to generate new diagnostic value well over a century after it was first described.
Preguntas frecuentes
Does the MCV blood test require fasting?
No. The MCV blood test is calculated as part of a complete blood count, and eating or drinking beforehand does not meaningfully change red blood cell size. You only need to fast if the same blood draw includes another test that requires it, such as a fasting glucose or cholesterol panel. If you are unsure, check the instructions given with your test order.
Can MCV change quickly, or does it stay stable?
El VCM es un valor bastante estable de un día para otro. Los glóbulos rojos viven aproximadamente 120 días, por lo que el tamaño promedio de las células en circulación no cambia drásticamente de la noche a la mañana. Los cambios significativos en el VCM suelen desarrollarse a lo largo de semanas o meses, a medida que los nuevos glóbulos rojos —formados según tu estado actual de hierro o vitaminas— van reemplazando gradualmente a los más viejos.
¿Qué significa que mi VCM sea normal pero aún me sienta mal?
Un VCM normal no descarta todos los problemas relacionados con los glóbulos rojos. Algunas personas tienen deficiencia de hierro temprana sin anemia, una combinación de deficiencias que se compensan entre sí, o una condición completamente diferente, como disfunción tiroidea o un trastorno del sueño. Si tu VCM es normal pero los síntomas persisten, coméntaselo a tu médico en lugar de asumir que la biometría hemática descartó todo.
¿Cómo cambia el VCM en los estudios de laboratorio durante el embarazo?
El embarazo provoca cambios fisiológicos reales en el VCM. En el segundo trimestre, el VCM puede disminuir ligeramente porque el volumen plasmático aumenta más rápido que la masa de glóbulos rojos, mientras que la demanda de hierro se incrementa. Más adelante en el embarazo, una ingesta insuficiente de folato puede elevar el VCM. Por eso se recomienda comúnmente la suplementación con hierro y ácido fólico durante todo el embarazo.
¿La etnia puede influir en lo que se considera un VCM normal?
Sí, en cierta medida. Las personas de ascendencia mediterránea, africana o del sudeste asiático pueden tener valores promedio de VCM ligeramente más bajos, lo que suele estar relacionado con una mayor prevalencia del rasgo de talasemia, una condición hereditaria generalmente benigna. Los médicos toman esto en cuenta para evitar estudios innecesarios cuando un VCM levemente bajo encaja con un patrón familiar conocido y no con un problema nuevo.
¿Un VCM bajo o alto siempre es motivo de preocupación?
No necesariamente. Un VCM levemente anormal sin síntomas y sin otros valores alterados en los estudios de sangre generalmente solo se vigila con un análisis de seguimiento en unos meses. Lo más importante es qué tan alejado está el valor del rango de referencia, si otros valores de los glóbulos rojos también están afectados y si tienes síntomas. Tu médico es quien mejor puede decidir si tu resultado específico requiere más estudios.
Fuentes
- VCM (Volumen Corpuscular Medio) — MedlinePlus, Biblioteca Nacional de Medicina (NIH) — https://medlineplus.gov/lab-tests/mcv-mean-corpuscular-volume/
- Análisis de sangre de Volumen Corpuscular Medio (VCM) — Cleveland Clinic — https://my.clevelandclinic.org/health/diagnostics/24641-mcv-blood-test
- Maner BS, Moosavi L. Mean Corpuscular Volume — StatPearls, NCBI Bookshelf (National Library of Medicine, NIH) — https://www.ncbi.nlm.nih.gov/books/NBK545275/
- Darshan BSD, Sampathila N, Bairy GM, et al. Differential diagnosis of iron deficiency anemia from aplastic anemia using machine learning and explainable Artificial Intelligence utilizing blood attributes — Scientific Reports, 2025 — https://doi.org/10.1038/s41598-024-84120-w
- Wang W, Ye R, Tang B, Qi Y. MultiThal-classifier, a machine learning-based multi-class model for thalassemia diagnosis and classification — Clinica Chimica Acta, 2024 — https://doi.org/10.1016/j.cca.2024.120025
Leer un solo valor marcado como el VCM rara vez cuenta toda la historia por sí solo. Combinarlo con otros resultados relacionados, como la hemoglobina, la ferritina o un panel completo de hierro, da una imagen mucho más clara de lo que está ocurriendo y te ayuda a entender —no a diagnosticar— lo que tu reporte podría estar indicando. AI DiagMe puede ayudarte a ver cómo encaja tu VCM junto con estos otros marcadores, traduciendo el patrón a un lenguaje sencillo antes de tu próxima cita. Está diseñado para ayudarte a entender tus resultados; no te diagnostica ni reemplaza a tu médico.
Entiende tus resultados de laboratorio con AI DiagMe
Obtén la lectura de tus resultados en minutos
Lecturas recomendadas
- Causas, síntomas y tratamientos del VCM bajo
- Cómo entender los niveles altos de VCM y sus causas
- Cómo leer los resultados de la biometría hemática (BH)
- Panel de estudios de hierro y qué significa cada marcador
- Rangos normales de análisis de sangre por panel
Glosario
| Término | Definición |
|---|---|
| Volumen corpuscular medio (VCM) | El volumen promedio de un solo glóbulo rojo, medido en femtolitros (fL). |
| Microcitosis | Un patrón de glóbulos rojos más pequeños de lo normal, generalmente por debajo de unos 80 fL. |
| Macrocitosis | Un patrón de glóbulos rojos más grandes de lo normal, generalmente por encima de unos 100 fL. |
| Biometría hemática (BH) | Un análisis de sangre común que mide los glóbulos rojos, los glóbulos blancos, las plaquetas y otros valores relacionados, incluido el VCM. |
| Hemoglobina | La proteína que contiene hierro dentro de los glóbulos rojos y que transporta el oxígeno por todo el cuerpo. |
| Anemia por deficiencia de hierro | La causa más frecuente de VCM bajo; ocurre cuando no hay suficiente hierro para sostener una producción normal de hemoglobina. |
| Folato (vitamina B9) | Una vitamina del complejo B necesaria para la síntesis de ADN durante la formación de glóbulos rojos; su deficiencia puede elevar el VCM. |
| Talasemia | Un grupo de enfermedades hereditarias que reducen la producción normal de hemoglobina y pueden disminuir el VCM. |
| Conteo de reticulocitos | Un análisis que mide cuántos glóbulos rojos nuevos e inmaduros están presentes, lo que refleja la actividad de la médula ósea. |
{kind=link}