


















A calcium blood test is one of the most common numbers on a routine lab report — and one of the most misread. On its own, a single calcium value tells only part of the story. Your body keeps blood calcium inside a very tight range using a small team of players: phosphate, parathyroid hormone (PTH), vitamin D, and an enzyme called alkaline phosphatase (ALP). Read together, these markers form what labs often call a bone and mineral panel, or “bone profile.”
This guide explains, in plain language, what each marker does, how they work as a system, and how to read them as a pattern instead of one number at a time. You will also find a results-interpretation table, the warning signs that deserve a doctor’s attention, and clear answers to the questions people ask most. None of this replaces your own clinician’s reading of your results.
What a calcium blood test actually measures
About 99% of your body’s calcium is stored in your bones and teeth. Only about 1% circulates in your blood, yet that small fraction is vital for your nerves, muscles, heart rhythm, and blood clotting. A calcium blood test measures that circulating amount — not the calcium locked inside your skeleton. So a normal result does not, by itself, confirm strong bones, and an abnormal one points to how calcium is being regulated rather than how dense your bones are.
Calcium usually appears on a routine comprehensive metabolic panel, which is why many people first see an unexpected calcium value without ever asking for it. A doctor may also order it on purpose — for example, if you have symptoms that could point to a parathyroid, kidney, thyroid, or bone problem, or to follow a known condition over time. Either way, when the number is off, doctors rarely act on it alone. They look at the supporting markers below to understand why it moved.
Total, ionized, and corrected calcium
Not all calcium tests measure the same thing, and the wording on your report matters.
- Total calcium is the standard measurement. It counts both the calcium attached to proteins (mainly albumin) and the free calcium floating in your blood. Most reports show this version; see our guide to the total calcium blood test for a closer look.
- Ionized (free) calcium measures only the active, unattached portion. It is more precise but needs special handling, so it is usually ordered when the total result is hard to interpret.
- Corrected calcium is a calculation that adjusts the total for your protein level. If your albumin is low, your true calcium may be higher than the raw number suggests, which is why the corrected (albumin-adjusted) calcium is often the figure that matters most.
The bone and mineral panel: five markers, one system
A bone and mineral panel groups the tests that keep blood calcium stable. Each marker answers a different question, and the value of the panel comes from reading them side by side.
Calcium — the tightly controlled mineral
Calcium is the headline number. Your body defends its blood calcium level fiercely, because both too much and too little can affect the heart, muscles, and brain. A stable result usually means the control system is working; a drifting one is a prompt to look at the regulators.
Phosphate (phosphorus) — calcium’s partner
Phosphate works hand in hand with calcium to build and repair bone. The two often move in opposite directions in the blood: when one rises, the other tends to fall. That mirror relationship is a useful clue, so a phosphate (phosphorus) blood test is frequently checked alongside calcium, especially when the kidneys or parathyroid glands are in question.
Parathyroid hormone (PTH) — the thermostat
PTH is the body’s calcium thermostat. Four tiny parathyroid glands in the neck release it whenever blood calcium dips. Because PTH and calcium are so closely linked, doctors almost always read the parathyroid hormone (PTH) test together with calcium — comparing the two is what reveals whether the glands are behaving appropriately. A second hormone, calcitonin, works in the opposite direction to help lower calcium.
Vitamin D (25-hydroxyvitamin D) — the absorption key
Vitamin D lets your gut absorb calcium from food. Without enough of it, you can eat plenty of calcium and still run low. The standard measurement is the vitamin D (25-hydroxyvitamin D) test, which reflects your overall vitamin D stores. Low vitamin D is one of the most common reasons calcium and PTH look abnormal together.
Alkaline phosphatase (ALP) — the bone-activity signal
ALP is an enzyme that rises when bone is being actively built or remodeled. It also comes from the liver, so an alkaline phosphatase (ALP) test is interpreted in context. Within a bone panel, a raised ALP can flag increased bone turnover. Magnesium is sometimes added too, because very low magnesium can stop PTH from working.
The table below summarizes the markers. Ranges are typical adult values for general orientation only — laboratories set their own reference ranges, so always compare each result to the range printed on your own report.
| Marker | What it measures | Typical adult range* | A high level may point to | A low level may point to |
|---|---|---|---|---|
| Calcium (total) | Calcium circulating in blood | ~8.5–10.5 mg/dL | Overactive parathyroid, some cancers, excess vitamin D | Low vitamin D, low albumin, kidney issues |
| Phosphate | Phosphorus in blood | ~2.5–4.5 mg/dL | Kidney disease, too much intake | Low vitamin D, overactive parathyroid |
| PTH (intact) | Parathyroid hormone | ~10–65 pg/mL | Parathyroid overactivity, low vitamin D | Underactive parathyroid, high calcium intake |
| Vitamin D (25-OH) | Vitamin D stores | varies; deficiency often <20 ng/mL | Usually supplement excess | Poor sun exposure, malabsorption, low intake |
| ALP | Bone/liver enzyme activity | ~44–147 IU/L | High bone turnover, liver issues | Less common; some genetic conditions |
*Reference ranges differ by lab, age, and pregnancy. Use your report’s ranges.
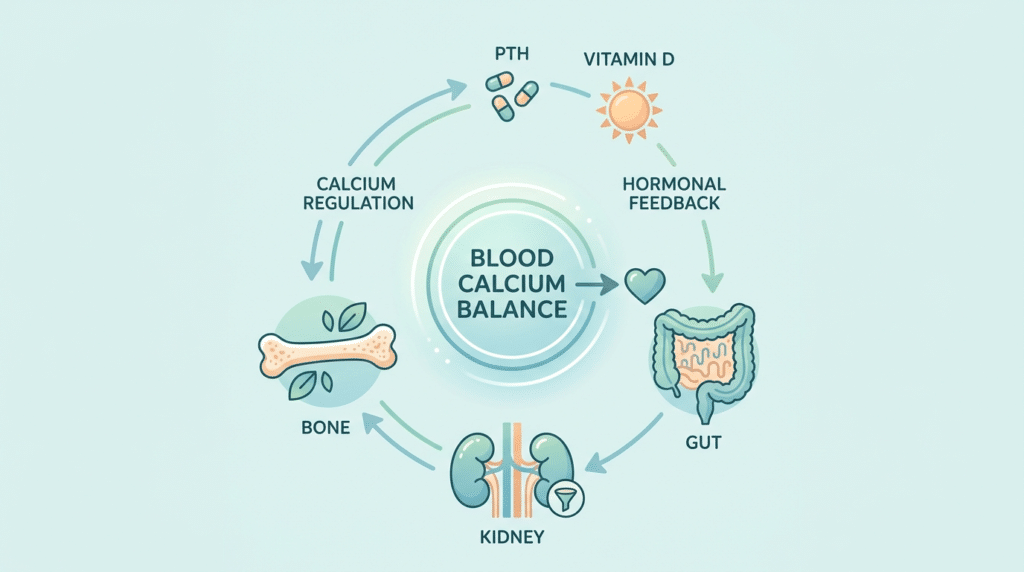
How the markers work together (the calcium loop)
The real power of this panel is the feedback loop that connects the markers. Picture a thermostat keeping a room at a set temperature.
When blood calcium falls, the parathyroid glands release more PTH. PTH then raises calcium three ways: it draws calcium out of bone, it tells the kidneys to hold on to calcium while flushing out phosphate, and it switches vitamin D into its active form so the gut absorbs more calcium from food. As calcium climbs back to normal, PTH eases off. The opposite happens when calcium runs high.
This is why the numbers only make sense together. A high calcium with a high PTH is very different from a high calcium with a low PTH, even though the calcium value is identical. The PTH tells you whether your body is driving the change or trying to correct it. A simple example: if vitamin D runs low for months, the gut absorbs less calcium, PTH climbs to compensate, and phosphate may drift down — so three markers move at once, all tracing back to a single cause.
Reading your results as a pattern
Clinicians rarely judge calcium alone. They read it as a pattern across calcium, PTH, phosphate, and vitamin D. The table below shows how common combinations are usually approached. It is a guide to the questions a doctor asks — not a diagnosis, and not a substitute for one.
| Calcium | PTH | Phosphate | What this pattern often suggests |
|---|---|---|---|
| High | High or “inappropriately” normal | Low/normal | Primary hyperparathyroidism is the most common explanation |
| High | Low | Normal/high | A cause outside the parathyroid (e.g. excess vitamin D or calcium intake, or another medical condition) — needs evaluation |
| Low | High | Low | Often vitamin D deficiency, prompting the glands to compensate |
| Low | Low | High | An underactive parathyroid; magnesium is usually checked too |
A few practical points. First, always start from the corrected (albumin-adjusted) calcium, since a low protein level can make calcium look falsely low. Second, a single odd result is often just that — labs repeat borderline values before acting. Third, ALP and your symptoms add context the numbers alone cannot.
One distinction explains many of these patterns: primary versus secondary changes. In a primary problem, a gland itself misbehaves — for instance, an overactive parathyroid that pushes calcium up on its own. In a secondary one, the gland is reacting correctly to something else, such as PTH rising to defend calcium when vitamin D is low. Same hormone, opposite meaning — which is exactly why the markers are read together. When in doubt, the safest next step is to bring the full panel to your doctor rather than interpreting one row in isolation. If you are new to lab reports, our guide on how to read your blood test results covers the basics.
What high or low calcium can mean
Common reasons for high calcium (hypercalcemia)
A high blood calcium level is called hypercalcemia. Most often it traces back to one or more overactive parathyroid glands. Other causes include certain cancers, some medical conditions, and taking too much calcium or vitamin D from supplements. According to the Mayo Clinic, mild cases sometimes have no symptoms at all and are picked up only on a routine test. Over time, untreated high calcium can weaken bones and contribute to kidney stones, which is one reason a persistent result is worth investigating.
Common reasons for low calcium (hypocalcemia)
A low level, or hypocalcemia, is frequently linked to low vitamin D, an underactive parathyroid, low magnesium, or kidney problems. Because so much blood calcium rides on albumin, a low protein level can also make calcium appear low even when the active (ionized) calcium is fine. That is exactly the situation the corrected calcium calculation is designed to catch.
Can you change your calcium levels?
Searches for how to lower calcium in the blood “naturally” are common, so it helps to be clear about what is realistic. In a healthy person, blood calcium is controlled by hormones, not by what you ate yesterday — your body adjusts absorption and storage to keep the level steady. Diet alone rarely moves it far.
What can shift your result is an underlying cause or an outside source. High doses of calcium or vitamin D supplements can push calcium up; staying well hydrated supports the kidneys in clearing excess. If you take supplements, it is worth knowing exactly how much calcium and vitamin D they contain, since combined doses from several products can add up without you noticing. If your calcium is abnormal, the goal is to find and treat the reason, not to chase the number with home remedies. Stopping supplements, adjusting medication, or treating a gland problem are decisions to make with a clinician — not on your own.
How the test is done and how to prepare
The sample is simple: a small blood draw from a vein in your arm, usually taking a few minutes. Preparation depends on what is being measured. Some labs ask you to fast before a calcium test, while a vitamin D test usually needs no special preparation. PTH is often drawn at the same time as calcium so the two can be compared directly.
Tell your provider about any supplements or medicines you take. Calcium salts (in some antacids and supplements), vitamin D, lithium, certain “water pills” (thiazide diuretics), and thyroid medication can all affect calcium results. Do not stop any prescribed medicine on your own — ask first.
When to see a doctor: warning signs
Most mild, one-off changes are simply something to review with your provider at your next visit. Some signs, though, deserve prompter attention — especially when they appear together with a clearly abnormal result.
Possible signs of high calcium include:
- Intense thirst and frequent urination
- Persistent nausea, vomiting, or constipation
- Bone pain or noticeable muscle weakness
- Trouble concentrating, confusion, drowsiness, or low mood
- A fast, fluttering, or irregular heartbeat (rare, and a reason to seek urgent care)
Possible signs of low calcium include:
- Tingling or numbness around the mouth, fingers, or toes
- Muscle cramps, twitching, or spasms
- In severe cases, fainting or seizures (seek urgent care)
If results are markedly abnormal, or symptoms are severe or worsening, contact a healthcare professional promptly. For ongoing kidney or parathyroid conditions, regular monitoring — sometimes including a kidney function panel — is part of routine care.
Glossary
- Albumin: The main protein in blood. About half of your calcium is attached to it, so albumin levels affect how calcium results are read.
- Alkaline phosphatase (ALP): An enzyme from bone and liver that rises when bone is being actively built or remodeled.
- Calcitonin: A hormone that helps lower blood calcium, working opposite to PTH.
- Corrected calcium: A calculation that adjusts total calcium for your albumin level to better reflect the true amount.
- Hypercalcemia: A higher-than-normal level of calcium in the blood.
- Hypocalcemia: A lower-than-normal level of calcium in the blood.
- Hyperparathyroidism: A condition in which the parathyroid glands make too much PTH.
- Ionized calcium: The free, active portion of blood calcium that is not attached to proteins.
- Parathyroid hormone (PTH): The hormone from the parathyroid glands that raises blood calcium when it falls.
- Phosphate (phosphorus): A mineral that partners with calcium to build bone and often moves opposite to it in the blood.
Frequently asked questions
What does high calcium in a blood test mean?
A high calcium level (hypercalcemia) means more calcium is circulating in your blood than expected. The most common reason is an overactive parathyroid gland, but other causes include certain medical conditions and taking too much calcium or vitamin D. A single high reading does not confirm any specific condition — many mild elevations come from dehydration, a recent supplement, or a non-fasting sample. Your doctor will usually repeat the test and check PTH and vitamin D to find the cause before drawing conclusions.
What is a normal blood calcium level?
For most adults, total calcium falls roughly between 8.5 and 10.5 mg/dL, though the exact range depends on the laboratory and your age. The number printed on your own report is the one to compare against, since labs calibrate their ranges differently. Because calcium rides on albumin, a low protein level can make the value look low; in that case the corrected (albumin-adjusted) calcium gives a more accurate picture than the raw figure.
Does a high calcium level mean cancer?
Not on its own. Most high calcium results come from an overactive parathyroid gland, not cancer, and many are mild and easily explained. Cancer is one of several possible causes of persistent hypercalcemia, particularly when PTH is low rather than high. A calcium number cannot diagnose anything by itself — only a doctor can interpret it alongside PTH, other tests, your history, and symptoms. If your level is persistently high, the right step is medical evaluation, not alarm.
What is PTH on a blood test?
PTH stands for parathyroid hormone, made by four small glands in your neck. It controls blood calcium: when calcium drops, PTH rises to bring it back up by acting on your bones, kidneys, and vitamin D. Because PTH and calcium are so tightly linked, they are almost always measured together. Comparing the two is what tells a clinician whether your parathyroid glands are responding normally or driving an abnormal calcium level themselves.
Do I need to fast for a calcium or vitamin D blood test?
It depends on the test and the laboratory. Some labs ask you to fast before a calcium test, partly because a recent calcium-rich meal can nudge the result. A vitamin D test usually needs no special preparation, and PTH is often drawn together with calcium. The safest approach is to follow the instructions your provider or lab gives you, and to mention any supplements or medicines beforehand, since several can affect calcium readings.
Can I check calcium, PTH and vitamin D at home?
Sample collection for these tests is done through a laboratory, either at a collection site or, in some areas, through a mobile service. What many people want help with afterward is understanding the results. A clear explanation of how your calcium, phosphate, PTH and vitamin D fit together can make a confusing report far easier to discuss with your doctor — though interpreting your specific situation, and any treatment, always remains a medical decision.
Sources
- Calcium Blood Test — MedlinePlus (U.S. National Library of Medicine)
- Vitamin D: Fact Sheet — NIH Office of Dietary Supplements
- Hypercalcemia: Symptoms and causes — Mayo Clinic
Further reading
- How to read your blood test results
- Total calcium blood test explained
- Vitamin D (25-OH) blood test
- Kidney function panel: how to read it
- Kidney stones: causes, symptoms and treatments
Understand your lab results with AI DiagMe
A bone and mineral panel only makes sense when its parts are read together — your calcium, phosphate (phosphorus), parathyroid hormone (PTH), and vitamin D each shape what the others mean. AI DiagMe turns that scattered set of numbers into a clear, plain-language explanation, so you walk into your next appointment knowing what to ask. It helps you understand your results; it does not diagnose and does not replace your doctor.
➡️ Get your results interpreted in minutes
{kind=link}