














Low TSH level means that your pituitary gland signals the thyroid to make less hormone than usual. In most adults, a low TSH level suggests excess thyroid hormone activity, but the result can mean different things depending on symptoms and other tests. This guide explains what causes a low TSH level, how clinicians evaluate it, common symptoms, treatment options, follow-up plans, and special considerations for pregnancy and older adults. You will learn practical steps to interpret results and when to seek specialist care.
Causes of low TSH level
The pituitary gland normally releases thyroid-stimulating hormone (TSH) to keep thyroid hormones balanced. When the body has too much thyroid hormone, the pituitary reduces TSH. In that setting, a low TSH level most often reflects primary hyperthyroidism. Common causes include autoimmune Graves disease, toxic nodules in the thyroid, and subacute or silent thyroiditis. Exogenous causes also lower TSH. People who take too much levothyroxine for hypothyroidism will show a low TSH. In addition, several drugs and illnesses change TSH levels.
Less commonly, problems in the pituitary or hypothalamus lead to an inappropriately low TSH despite low thyroid hormones. This central hypothyroidism requires a different diagnostic and treatment approach. Critical illness and certain tests or supplements can also alter TSH temporarily.
Common causes of low TSH level
- Graves disease producing excess thyroid hormone.
- Toxic multinodular goiter or a toxic adenoma.
- Subacute, silent, or postpartum thyroiditis causing hormone release.
- Overreplacement with thyroid hormone medication.
- Early pregnancy, when hCG lowers TSH transiently.
- Non-thyroidal illness (acute severe illness) that suppresses TSH.
Medications and supplements that affect TSH
- Excess levothyroxine will lower TSH.
- Amiodarone can produce variable thyroid effects.
- High-dose glucocorticoids and dopamine reduce TSH secretion.
- Biotin supplements can interfere with some lab assays and give falsely low results.
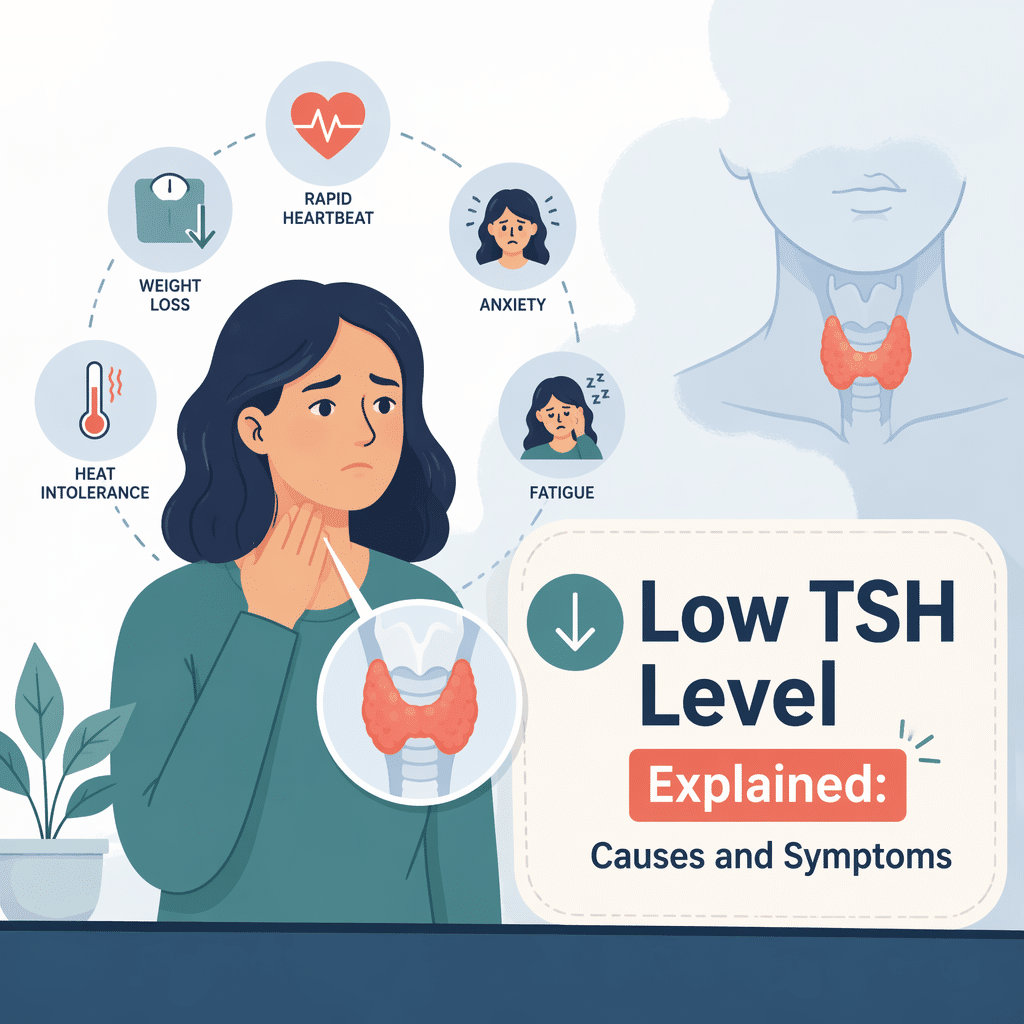
Symptoms and signs of low TSH level
Symptoms depend on the underlying cause. When a low TSH level accompanies high thyroid hormones, typical hyperthyroid symptoms appear. People often report weight loss, a racing heart, tremor, heat intolerance, and anxiety. They may also have irregular periods, increased bowel movements, and muscle weakness. In contrast, a low TSH with low thyroid hormones suggests central hypothyroidism. In that case, patients feel cold, gain weight, and move more slowly.
Some people with a low TSH level show no symptoms. Mild biochemical changes appear on screening tests, and a clinician might observe them before treatment. Therefore, doctors always interpret TSH together with free T4 and free T3 levels and the clinical picture.
How doctors diagnose a low TSH level
Clinicians start by repeating abnormal results to confirm a persistent low TSH. Next, they measure free T4 and often free T3. If TSH is low with high free T4 or free T3, the team evaluates for primary hyperthyroidism. If TSH is low but free T4 is low or normal, they consider central causes or laboratory interference.
Doctors also review medications, supplements, and recent illnesses. They ask about symptoms, family history, and recent pregnancy. Depending on the suspected cause, they may order thyroid-stimulating immunoglobulin tests, thyroid ultrasound, or radioactive uptake testing. Referral to an endocrinologist helps when tests remain unclear or when pituitary disease might explain the results.
Lab tests for low TSH level
- Repeat TSH to confirm the finding.
- Measure free T4 and free T3 for hormone activity.
- Consider thyroid antibody tests when autoimmune disease is likely.
- Use thyroid ultrasound when nodules or structural disease appear likely.
- Reserve pituitary imaging if central hypothyroidism or other pituitary signs exist.
When to repeat testing and additional tests
Repeat TSH after a few weeks when illness or medicines may have affected results. Also repeat after adjusting thyroid medication. If tests remain abnormal, pursue targeted imaging or specialist referral. Avoid treating a single, isolated low value without clinical context.
Treatment options for low TSH level
Treatment depends on the diagnosis and symptom severity. For overt hyperthyroidism, clinicians choose one of three main strategies. They may use antithyroid drugs to reduce hormone production. Alternatively, they may recommend radioactive iodine to ablate thyroid tissue. Surgery becomes an option for large goiters, suspicious nodules, or when rapid control is necessary. For thyroiditis, teams often use beta blockers for symptom control and recommend anti-inflammatory measures while the gland recovers.
When a low TSH level reflects excess replacement hormone, clinicians reduce the levothyroxine dose. For central hypothyroidism, doctors replace thyroid hormone but monitor free T4 rather than relying on TSH. In every case, teams individualize care by age, cardiac risk, pregnancy status, and other health issues.
Medication options for low TSH level
- Methimazole usually controls production in most adults.
- Propylthiouracil suits special situations, such as early pregnancy.
- Beta blockers quickly relieve palpitations, tremor, and anxiety.
- Levothyroxine adjustments correct overreplacement when it causes low TSH.
When surgery or radioactive iodine is considered
Surgery suits people with large obstructive goiters, suspicious nodules, or those who want a definitive fix. Radioactive iodine offers a non-surgical option to destroy overactive thyroid tissue. Teams discuss risks and benefits, especially in older adults and pregnant people.
Monitoring and long-term management
After treatment starts, clinicians schedule regular testing to track thyroid hormone levels. TSH can take several weeks to settle after medication changes. Therefore, doctors usually repeat tests every 6 to 8 weeks during dose adjustments. Once stable, many patients shift to testing every 6 to 12 months.
Long-term monitoring should also assess bone density and heart health. Untreated or prolonged hyperthyroidism increases the risk of atrial fibrillation and bone loss. Teams address these risks with appropriate screening and management. In addition, clinicians counsel patients about symptoms that require urgent attention, such as a very fast heartbeat or sudden weakness.
Low TSH level in pregnancy and special groups
Pregnancy changes thyroid physiology. During the first trimester, hCG can transiently lower TSH. Because thyroid hormones influence fetal development, clinicians test and manage thyroid disease more actively during pregnancy. They tend to treat overt hyperthyroidism and adjust levothyroxine carefully for women with hypothyroidism.
Older adults may show fewer classic hyperthyroid symptoms but higher risk of heart rhythm problems. Children and teens with low TSH require prompt evaluation because thyroid disease can affect growth and development. Always inform the care team about pregnancy plans, age-related risks, and other health conditions.
Preventing and reducing risk
You can reduce risk for a low TSH level caused by overreplacement. First, follow dosing instructions for thyroid medication. Second, avoid self-adjusting doses without testing. Third, review new medications and supplements with your clinician, because some lower TSH or interfere with assays. Finally, maintain regular follow-up and repeat testing when clinicians recommend it.
Frequently Asked Questions (FAQ)
Q: What does a low TSH level mean if I feel fine?
A: A low TSH level may reflect early or mild thyroid overactivity or a temporary change from illness or medication. Your clinician will check free T4 and free T3 and may repeat tests before deciding on treatment.
Q: Can pregnancy cause a low TSH level?
A: Yes. In early pregnancy, hCG often lowers TSH temporarily. Clinicians interpret results using pregnancy-specific reference ranges and monitor thyroid hormones closely.
Q: How soon will treatment change my TSH level?
A: TSH usually shifts slowly. After starting or changing therapy, you may need 6 to 8 weeks to see a stable TSH response. Doctors often adjust doses based on that timing.
Q: Could supplements give a false low TSH result?
A: Yes. High biotin intake can interfere with some lab tests and produce misleading results. Tell your clinician about supplements before testing.
Q: When should I see an endocrinologist for a low TSH level?
A: Ask for specialist input if results stay abnormal, if you have symptoms affecting daily life, if you are pregnant, or if pituitary disease might explain the findings.
Q: Is a low TSH level dangerous?
A: It depends. Untreated hyperthyroidism raises risks for heart rhythm problems and bone loss. Early evaluation and tailored treatment reduce long-term risks.
Glossary of Key Terms
- TSH: Thyroid-stimulating hormone from the pituitary that regulates thyroid function.
- Free T4: The active form of thyroxine circulating in blood.
- Free T3: The active triiodothyronine hormone produced by the thyroid and by conversion from T4.
- Hyperthyroidism: A state of excess thyroid hormone activity with related symptoms.
- Central hypothyroidism: Low thyroid hormone levels due to pituitary or hypothalamic dysfunction, often with low TSH.
- Thyroiditis: Inflammation of the thyroid that can release stored hormone.
- hCG: Human chorionic gonadotropin, a pregnancy hormone that can lower TSH.
- Euthyroid sick syndrome: Temporary changes in thyroid tests during severe illness that do not reflect true thyroid disease.
Understand Your Lab Test Results with AI DiagMe
Understanding a low TSH level starts with clear interpretation of lab patterns and the clinical context. AI DiagMe helps you translate lab numbers into plain-language explanations and next-step suggestions. Use the tool to explore what a low TSH level might mean for you and to prepare informed questions for your clinician.
➡️ Analyze Your Lab Results with AI DiagMe Now
{kind=link}