


















Ett proteinelektroforestest sorterar de många proteinerna i ditt blod i separata grupper och mäter sedan hur mycket du har av varje grupp. Om din laboratorierapport nämner albumin, alfa-, beta- eller gammaglobuliner – eller en "M-spike" – kommer alla dessa siffror från detta test, och tillsammans ger de en ögonblicksbild av ditt immunförsvar, din lever och dina njurar. Immunglobuliner, de antikroppar som din kropp använder för att bekämpa infektioner, är en central del av vad det avslöjar. Den här guiden förklarar, i ett enkelt språk, vad varje proteinband på din rapport betyder, hur immunglobuliner passar in, den avgörande skillnaden mellan ett "polyklonalt" och ett "monoklonalt" resultat och när ett onormalt värde är värt att diskutera med din läkare.
Vad ett proteinelektroforestest mäter
Ditt blod innehåller hundratals olika proteiner. Ett proteinelektroforestest placerar ett litet prov i en gel och låter en elektrisk ström passera genom det. Eftersom proteiner skiljer sig åt i storlek, form och elektrisk laddning, färdas de genom gelen med olika hastigheter och radas upp i separata rader. band (även kallad bråkdelarLaboratoriet mäter sedan hur mycket protein som finns i varje band.
De flesta rapporter grupperar allt i två breda familjer: albumin, det enskilt vanligaste proteinet, och globuliner, en blandad familj som inkluderar transportproteiner, inflammationsproteiner och dina antikroppar.
När testet körs på blodserum kallas det serumproteinelektrofores (SPEP); när det körs på urin kallas det urinproteinelektrofores (UPEP). Många laboratorier rapporterar också totalt protein figur och albumin-till-globulin (A/G)-förhållande, en enkel jämförelse som kan antyda om proteinproduktionen eller -förlusten är i obalans.
Resultat visas vanligtvis på två sätt samtidigt: som en kurva, eller spårning, där varje grupp av proteiner bildar en topp, och som en lista med siffror som anger mängden i varje fraktion – ofta både som en procentandel av det totala proteinet och som en koncentration. En läkare kan beställa testet när rutinmässiga blodprover visar ett ovanligt högt eller lågt totalt protein, när det finns tecken på inflammation eller ett möjligt immunproblem, eller för att hålla ett öga på ett känt tillstånd över tid. Eftersom fraktionerna är länkade kan ett band se onormalt ut helt enkelt för att ett annat har stigit eller sjunkit, vilket är anledningen till att hela mönstret läses tillsammans snarare än en enskild siffra för sig.
Proteinfraktionerna i din rapport, en efter en
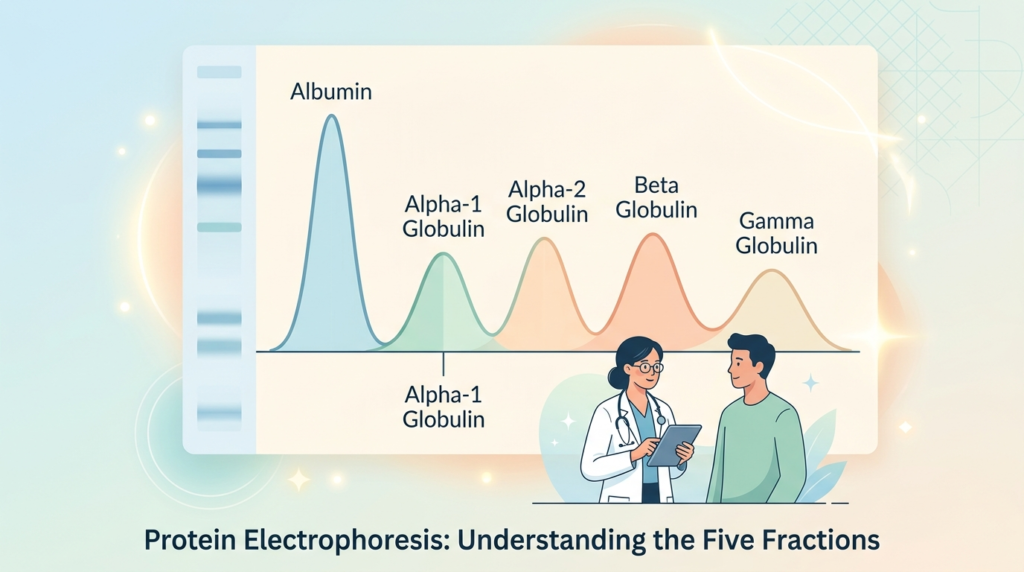
En standardrapport för serumproteinelektrofores visar fem band. Varje band innehåller olika proteiner, så en förändring i en fraktion pekar på en annan del av kroppen. Här är vad varje band representerar och vad en ovanlig nivå kan antyda. Tabellen nedan är endast en snabb orientering; dessa är allmänna tendenser, och betydelsen av ett givet mönster beror på din fullständiga kliniska bild.
| Fraktion | De viktigaste proteinerna den innehåller | En högre nivå kan föreslå | En lägre nivå kan antyda |
|---|---|---|---|
| Albumin | Albumin | Uttorkning | Leversjukdom, proteinbrist i njurarna, undernäring, inflammation |
| Alfa-1 | Alfa-1-antitrypsin | Akut inflammation | En genetisk alfa-1-antitrypsinbrist |
| Alfa-2 | Haptoglobin, alfa-2-makroglobulin | Inflammation, proteinförlust i njurarna | Nedbrytning av röda blodkroppar (haptoglobinfall) |
| Beta | Transferrin, komplementproteiner | Järnbrist (transferrin stiger) | Undernäring, inflammation |
| Gamma | Immunglobuliner (antikroppar) | Infektion, inflammation, ett monoklonalt protein | Ett försvagat immunförsvar (låga antikroppar) |
Albumin
Albumin produceras av levern och håller vätska inuti dina blodkärl samtidigt som det transporterar hormoner, vitaminer och läkemedel. En låg albuminnivå återspeglar oftast leversjukdom, proteinförlust genom njurarna, dålig näring eller pågående inflammation. En hög albuminnivå är vanligtvis ett tecken på uttorkning snarare än sjukdom. Eftersom albumin produceras i levern kan ett stadigt lågt värde vara en tidig ledtråd till långvariga lever- eller njurproblem, och det rör sig ofta i motsatt riktning mot inflammation.
Alfa-1 och alfa-2 globuliner
De alfa-1-globuliner består till stor del av ett protein som kallas alfa-1-antitrypsin, vilket stiger vid inflammation. Ett lågt alfa-1-band kan ibland tyda på en genetisk sjukdom som påverkar lungorna och levern. alfa-2-globuliner inkluderar haptoglobin och alfa-2-makroglobulin; detta band tenderar att stiga vid inflammation och när njurarna läcker protein, och haptoglobin sjunker när röda blodkroppar bryts ner snabbare än normalt. Båda alfabanden är en del av kroppens snabba reaktion på stress och vävnadsskador, så de stiger ofta tillsammans under en akut sjukdom och stabiliseras igen när man tillfrisknar.
Betaglobuliner
De beta-globuliner bär proteiner som transferrin, som transporterar järn, och flera komplementproteiner som stödjer immunförsvaret. Transferrin stiger ofta när kroppen har järnbrist, så detta band kan förskjutas vid järnbrist. Komplementproteinerna i detta band är en del av immunsvaret, och förändringar här avläses tillsammans med gammabandet snarare än på egen hand.
Gammaglobuliner
De gammaglobuliner är det band som läkare undersöker noggrannare, eftersom det är där din immunoglobuliner — dina antikroppar — dyker upp. En bred ökning här är vanlig och vanligtvis reaktiv. En skarp, smal topp är det fynd som föranleder ytterligare tester, vilket förklaras nedan. Ett lågt gammaband spelar också roll: det kan tyda på ett försvagat immunförsvar som inte kan producera tillräckligt med antikroppar, ibland kallat hypogammaglobulinemi.
Immunglobuliner: IgG, IgA och IgM
Immunglobuliner är Y-formade proteiner som immunsystemet producerar för att känna igen och neutralisera bakterier. Tre huvudklasser mäts i vardagen, och var och en har en annan funktion.
- IgG är den vanligaste antikroppen och bär ditt långsiktiga immunminne; det är den typ som byggs upp efter infektioner och vaccinationer. Läs mer i vår guide till immunoglobulin G (IgG).
- IgA skyddar kroppens slemhinnor, såsom tarm, luftvägar och saliv, där bakterier först försöker ta sig in. Se vår artikel om immunoglobulin A (IgA).
- IgM är den största antikroppen och den första kroppen producerar när den drabbas av en ny infektion, vilket gör att den kan signalera en nyligen inträffad sjukdom. Läs mer om immunoglobulin M (IgM).
Dessa antikroppar kan synas i dina resultat på två sätt. De utgör större delen av gammabandet vid elektrofores, och de kan också mätas en och en som kvantitativa immunoglobuliner. En förhöjd nivå av en klass återspeglar ofta infektion eller inflammation, medan en låg nivå kan tyda på ett försvagat immunförsvar som kan behöva specialistgranskning.
Det är normalt att immunglobulinnivåerna varierar med åldern. Nyfödda börjar med antikroppar som de ärvs från sin mor och bygger upp sin egen förrådskapacitet under de första levnadsåren, så barn jämförs med åldersspecifika intervall snarare än vuxna. Hos vuxna kan en ihållande låg nivå av en eller flera klasser tyda på en immunbrist, medan en förhöjd nivå pekar tillbaka på orsakerna som ses i gammabandet: infektion, inflammation eller, mer sällan, en monoklonal process. Som alltid tolkas ett enda värde tillsammans med resten av dina resultat.
Polyklonal vs monoklonal: den viktigaste skillnaden
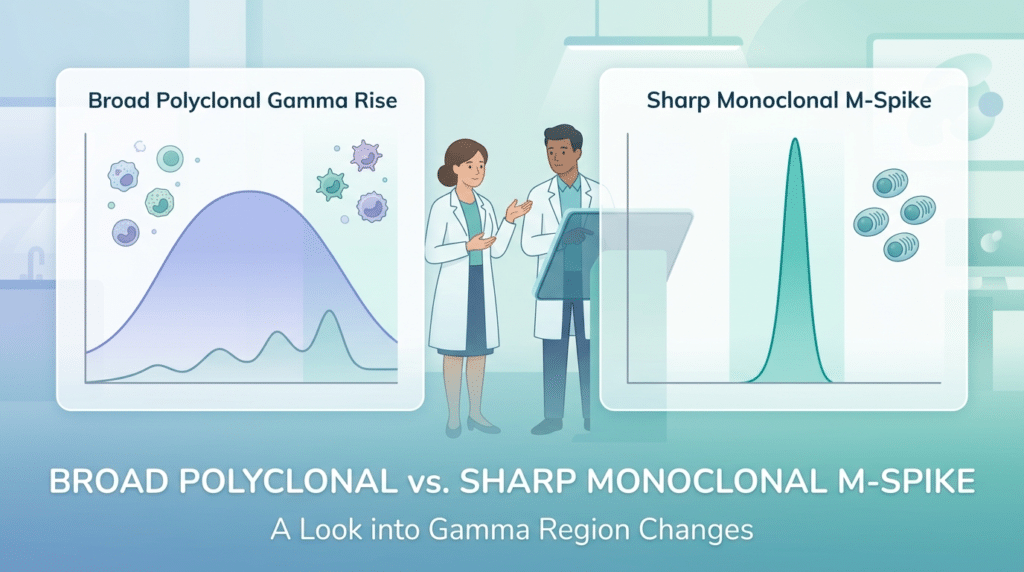
Om ett enda koncept från din rapport är värt att förstå, så är det skillnaden mellan en polyklonal och en monoklonal ökning i gammabandet. De ser olika ut på grafen och betyder väldigt olika saker.
Ett polyklonalt mönster (en bred stigning)
En polyklonal ökning sker när många olika antikroppsproducerande celler svarar samtidigt. På kurvan framträder det som en bred, rundad ökning snarare än en skarp topp. Detta mönster är vanligtvis reaktiv och visar sig med infektioner, kronisk inflammation, leversjukdom och autoimmuna tillstånd. Till exempel kan en långvarig infektion, ett autoimmunt tillstånd som reumatoid artrit eller lupus, och kronisk leversjukdom alla lyfta hela gammabandet samtidigt, eftersom kroppen producerar många olika antikroppar som svar. Det är vanligt och tyder i sig sällan på cancer. Vår artikel om en hög globulinnivå behandlar de vardagliga orsakerna mer i detalj.
Ett monoklonalt mönster (en skarp spik)
En monoklonal ökning kommer från en enda klon av plasmaceller som överproducerar en identisk antikropp. På spårningen framträder detta som en hög, smal topp som kallas en M-spik eller M-protein. Eftersom det återspeglar en cellinje som arbetar övertid, undersöks ett monoklonalt fynd vidare. Det kan kopplas till ett vanligt och ofta ofarligt fynd som kallas MGUS (monoklonal gammopati av obestämd betydelse), som enkelt övervakas, eller tillstånd som multipelt myelom eller Waldenströms makroglobulinemi.
Storleken på topparna och typen av antikropp spelar båda roll. Många människor, särskilt när de blir äldre, upptäcks ha ett litet monoklonalt protein som aldrig orsakar problem och helt enkelt kontrolleras då och då. En större topp, eller en som upptäcks tillsammans med symtom eller andra onormala resultat, leder till en remiss så att en specialist kan undersöka närmare. Att hitta ett M-protein är därför en anledning till utredning, inte en diagnos i sig.
Hur proteinelektrofores markerar det
Proteinelektrofores är en screeningsteg, inte en slutgiltig diagnos. När en möjlig M-spik uppträder bekräftar laboratoriet den och identifierar den med ett test som kallas immunfixering, och mäter antikroppsfragmenten involverade med fri ljuskedja testning. Vår guide till förhållandet mellan kappa/lambda-fria lätta kedjor förklarar hur uppföljningen fungerar.
Testerna som vanligtvis utförs med elektrofores
Serumproteinelektrofores går sällan ensamt. När en läkare vill ha en tydlig bild av dina antikroppar beställer de ofta en liten grupp tester tillsammans, och att se dem alla på ett och samma formulär kan vara förvirrande. Här är vad varje test lägger till:
- Immunfixering (IFE): identifierar den exakta typen av en onormal antikropp när elektrofores visar en topp.
- Fria lätta kedjor (kappa och lambda): mäter små antikroppsfragment och deras förhållande, vilket hjälper till att upptäcka och övervaka plasmacellsstörningar.
- Kvantitativa immunglobuliner: rapportera mängden IgG, IgA och IgM individuellt snarare än som ett enda band.
- Urinproteinelektrofores (UPEP): kontrollerar om det finns onormala proteiner som njurarna utsöndrar i urinen.
Tillsammans låter dessa tester en specialist avgöra om en förändring är en ofarlig reaktion eller något som behöver uppföljas. Att se flera av dessa namn på ett och samma laboratorieformulär betyder inte att något är fel; det betyder vanligtvis att din läkare vill ha en fullständig bild av dina antikroppar i en enda testomgång.
Urinproteinelektrofores (UPEP)
Urinversionen av testet letar efter monoklonala proteiner som har passerat från blodet till urinen. Historiskt kallades dessa Bence Jones-proteiner, och de är helt enkelt fria lätta kedjor som förekommer i urinen. UPEP är särskilt användbart när läkare undersöker njurarna eller följer ett plasmacellstillstånd. Eftersom lätta kedjor är små kan de slinka genom njurens filter in i urinen även när blodresultatet ser anmärkningsvärt ut, så att testa blod och urin tillsammans ger en mer fullständig bild än att testa endera av dem var för sig. Om dina urinresultat också visar protein, kan du läsa vår artikel om protein i urinen förklarar de vanligaste orsakerna och nästa steg.
När du ska prata med din läkare om resultaten
De flesta lätt avvikande resultat är inte en anledning till oro. En blygsam, polyklonal ökning av gammabandet återspeglar ofta helt enkelt en nyligen genomförd infektion eller pågående inflammation, och många människor har resultat som återgår till det normala när de tillfrisknar. Även ett bekräftat monoklonalt protein hålls ofta under enkel observation, med regelbundna blodprover snarare än behandling, när det är litet och inte orsakar några symtom.
Vissa fynd förtjänar dock ett snabbt samtal med din läkare:
- En M-spike eller monoklonalt protein rapporteras om dina resultat.
- Du har benvärk eller en oförklarlig fraktur.
- Du känner ihållande, oförklarlig trötthet eller har fått höra att du är anemisk.
- Du får frekventa eller svårläkande infektioner.
- Du märker skummande urin eller andra tecken på njurbelastning.
- Du har oförklarlig viktminskning, domningar eller stickningar.
Oavsett vad siffrorna visar är en enda rapport bara en del av bilden. En läkare tolkar den tillsammans med dina symtom, din historia och eventuella andra tester innan han drar slutsatser, och att jämföra ett resultat med tidigare resultat säger ofta mer än en enda ögonblicksbild. Av den anledningen är det bäst att inte ställa självdiagnos enbart utifrån siffrorna.
Ordlista
- Albumin: Det vanligaste proteinet i blodet, produceras av levern; det håller vätska inuti blodkärlen och transporterar många ämnen.
- Bence Jones-protein: monoklonala fria lätta kedjor som passerar in i urinen; ett äldre namn för vad urinelektrofores kan detektera.
- Fria lätta kedjor (kappa och lambda): små antikroppsfragment; mätning av kappa-till-lambda-förhållandet hjälper till att upptäcka eller övervaka plasmacellsstörningar.
- Gammaglobuliner: den grupp av blodproteiner som innehåller de flesta av dina antikroppar (immunoglobuliner).
- Immunfixering (IFE): ett uppföljande laboratorietest som identifierar den exakta typen av en onormal antikropp som ses vid elektrofores.
- Immunglobulin (antikropp): ett protein som immunsystemet producerar för att känna igen och bekämpa bakterier; de viktigaste typerna är IgG, IgA och IgM.
- M-spik (M-protein): en skarp, smal topp vid elektrofores orsakad av att en klon av plasmaceller producerar en enda antikropp; det föranleder ytterligare tester.
- MGUS (monoklonal gammopati av obestämd betydelse): ett vanligt, vanligtvis ofarligt fynd av ett litet monoklonalt protein som övervakas över tid.
- Monoklonal gammopati: närvaron av ett M-protein; “monoklonalt” betyder att det kommer från en enda cellinje.
- Polyklonal gammopati: en bred ökning av många antikroppar samtidigt, vanligtvis från infektion, inflammation eller leversjukdom snarare än cancer.
Vanliga frågor
Vad används serumproteinelektrofores för att diagnostisera?
Testet är huvudsakligen ett screenings- och övervakningsverktyg. Genom att mäta proteinbalansen i blodet kan det indikera sjukdomar i immunförsvaret, kronisk inflammation, lever- och njursjukdomar och tecken på en plasmacellssjukdom såsom multipelt myelom. Det ger vanligtvis inte en slutgiltig diagnos i sig. Istället pekar det läkare mot det område de ska undersöka, och alla ovanliga mönster – särskilt en monoklonal topp – bekräftas med uppföljningstester innan någon slutsats dras.
Behöver jag fasta före ett proteinelektroforestest?
För de flesta behövs ingen särskild förberedelse för ett proteinelektroforesblodprov, och du kan vanligtvis äta och dricka normalt. Vissa laboratorier eller läkare kan be dig att följa specifika instruktioner, särskilt om provet tas samtidigt som andra tester som kräver fasta. Det säkraste tillvägagångssättet är att följa de exakta anvisningarna på ditt labbrev eller att fråga teamet som tar ditt blod. Berätta för dem om eventuella läkemedel eller nyligen genomförda vaccinationer, eftersom dessa ibland kan påverka proteinnivåerna.
Vad betyder en hög gammaglobulinnivå?
En hög gammaglobulinnivå återspeglar extra antikroppar i blodet, men formen på ökningen spelar större roll än antalet. En bred, polyklonal ökning betyder vanligtvis att ditt immunförsvar reagerar på en infektion, inflammation, leversjukdom eller ett autoimmunt tillstånd. En smal, monoklonal topp kommer från en enda cellinje och undersöks vidare. Eftersom samma rubriksiffra kan ha mycket olika betydelser läser din läkare den tillsammans med elektroforeskurvan och dina andra resultat.
Vad är skillnaden mellan proteinelektrofores och immunfixering?
Proteinelektrofores separerar och mäter de breda grupperna av proteiner i ditt blod och används för att screena för ett onormalt mönster. Immunfixering är ett mer detaljerat uppföljningstest som identifierar den exakta typen av antikropp när elektrofores antyder ett monoklonalt protein. Enkelt uttryckt väcker elektrofores frågan genom att upptäcka ett ovanligt band, och immunfixering besvarar den genom att namnge den specifika antikroppen som är involverad. De två testerna används ofta i sekvens snarare än som alternativ.
Är ett onormalt proteinelektroforesresultat alltid allvarligt?
Nej. Många avvikande resultat är milda och reaktiva, vilket återspeglar en nyligen genomförd infektion eller pågående inflammation, och de försvinner ofta när man återhämtar sig. Även när ett monoklonalt protein hittas är den vanligaste förklaringen MGUS, ett låggradigt fynd som vanligtvis är ofarligt och bara övervakas över tid. Ett litet antal resultat kräver närmare uppmärksamhet, vilket är anledningen till att uppföljningstester finns. Din läkare kommer att förklara var just ditt resultat ligger och om något mer behövs.
Hur lång tid tar resultatet av proteinelektrofores?
Tidpunkten varierar mellan laboratorier, men resultaten är vanligtvis klara inom några arbetsdagar. När uppföljningssteg som immunfixering eller gratis lättkedjetestning läggs till kan hela uppsättningen ta lite längre tid att slutföra. Din läkare eller laboratoriet som bearbetade ditt prov kan ge dig den mest exakta tidsramen för dina resultat.
Källor
- Proteinelektrofores genom immunofixeringsblodtest — MedlinePlus (US National Library of Medicine)
- Serumproteinelektrofores — Cleveland Clinic
- Elektrofores — StatPearls, NCBI-bokhyllan (National Institutes of Health)
Vidare läsning
- Läs blodprovsresultaten: en enkel guide
- Albumin-globulin-förhållandet: tolkning och nivåer
- Gammaglobuliner: tolkning av höga eller låga nivåer
- Hög globulinnivå: orsaker och behandlingar
- Protein i urinen: orsaker, symtom och risker
Förstå dina labresultat med AI DiagMe
Att läsa en proteinelektroforesrapport kan kännas överväldigande när den listar albumin, alfa-, beta- och gammabanden, immunoglobuliner (dina IgG-, IgA- och IgM-antikroppar) och kanske fria lätta kedjor, allt på en gång. AI DiagMe hjälper dig att förstå dessa värden på ett enkelt språk, så att du kommer till ditt möte med tydliga frågor snarare än oro. Den är byggd för att hjälpa dig. förstå dina resultat, inte för att ställa diagnos, och det ersätter aldrig din läkares bedömning.
➡️ Få dina resultat tolkade på några minuter

{kind=link}