














An albumin blood test measures the main protein your liver releases into circulation, and the result helps explain your nutrition, liver, and kidney status in one number. Many people first encounter this marker on a routine metabolic panel and want to know quickly whether their value is reassuring or worth discussing further. This guide walks through what albumin does in the body, what counts as a normal range, why levels drop or rise, and how doctors combine this result with other markers before drawing conclusions. You will also find a comparison table, a glossary, recent research, and a short FAQ to round out the picture, so you can approach your next appointment with clear, specific questions.
What albumin does in the body
Albumin is a protein made almost entirely by the liver, and it accounts for roughly half of all the protein circulating in your blood plasma. Once released into the bloodstream, it takes on several jobs that keep your internal environment stable and your organs supplied with what they need.
Picture your bloodstream as a busy delivery network. Albumin acts like a fleet of small carrier vehicles that keep fluid inside the vessels, ferry hormones and vitamins to their destinations, and help buffer your blood chemistry. Losing a large share of this fleet, whether from reduced production or increased loss, changes how well that network functions.
Four core functions worth knowing
- Maintaining oncotic pressure, which keeps fluid inside your blood vessels instead of leaking into surrounding tissue and causing swelling.
- Transporting substances such as thyroid hormones, vitamins A, D, E, and K, fatty acids, bilirubin, and many medications through the bloodstream.
- Buffering blood pH, helping your body maintain the narrow acid-base balance that cells require to function normally.
- Providing antioxidant support by binding and neutralizing certain reactive molecules that would otherwise damage tissue.
Because it touches so many systems, doctors order this marker for a wide range of reasons. It routinely appears in liver function panels, nutritional assessments, and comprehensive metabolic panels, and clinicians frequently review it alongside kidney and inflammation markers. A single albumin value, taken alone, rarely tells the whole story; it works best as one piece of a broader clinical picture that your provider assembles over time.
Normal albumin range and how results are reported
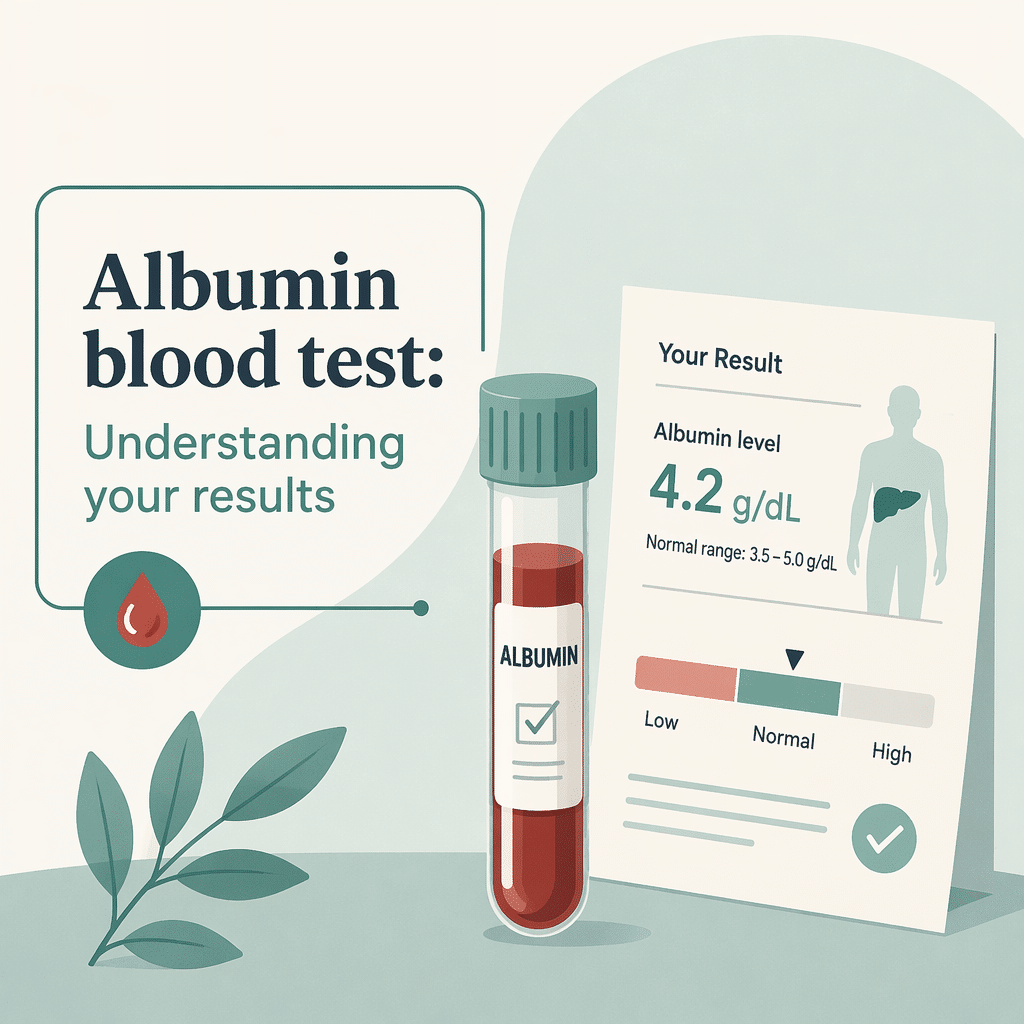
On a typical lab report, albumin appears in the biochemistry or protein section, next to a reference interval established by that specific laboratory. A standard adult reference range runs from roughly 3.5 to 5.0 grams per deciliter (g/dL), which converts to about 35 to 50 grams per liter (g/L). Some labs use slightly different cutoffs depending on their equipment and local population, so always check the interval printed on your own report rather than relying on a single universal number.
A result typically looks like this: ALBUMIN 4.2 g/dL, reference range 3.5 to 5.0 g/dL. Labs often add a flag, such as an arrow or a color code, when a value falls outside that printed range.
Quick checklist when reviewing your result
- Confirm whether your value sits inside the laboratory’s own reference range, not a number from an unrelated source.
- Check whether an arrow, color, or asterisk marks the result as abnormal.
- Compare the current figure with any previous albumin tests to spot a meaningful trend.
- Note whether related results, such as total protein, liver enzymes, or kidney markers, are also flagged.
- Consider recent context, including illness, surgery, pregnancy, or significant dietary changes, that could explain a temporary shift.
Causes of low albumin (hypoalbuminemia)
A below-range result, called hypoalbuminemia, is the more common and generally more clinically significant finding. Several distinct mechanisms can drive it down, and identifying which one applies to you usually requires additional testing rather than the albumin value alone.
Liver-related causes
Since the liver manufactures nearly all circulating albumin, conditions that damage liver tissue, such as cirrhosis or chronic hepatitis, can directly reduce output. A low reading in this context often parallels changes in other liver markers, so clinicians typically request a full liver panel to clarify the picture. Reviewing your AST (SGOT) test results alongside your ALT levels helps a clinician judge whether ongoing liver cell injury, rather than reduced synthetic capacity alone, is contributing to a low albumin value.
Kidney-related causes
Nephrotic syndrome and other conditions that damage the kidney’s filtering units allow this protein to leak into urine, quickly lowering blood levels even when the liver keeps producing normally. Doctors investigating this pathway usually order a urine albumin-to-creatinine ratio alongside standard kidney function tests, and they often check your अनुमानित ग्लोमेरुलर फिल्ट्रेशन दर (ईजीएफआर) to see how efficiently the kidneys are filtering overall.
Nutritional causes
Because albumin production depends on adequate protein and calorie intake, malnutrition, prolonged restrictive dieting, or malabsorption conditions such as celiac disease can gradually reduce levels. This nutritional pathway is one reason clinicians increasingly discuss albumin as a broader marker of overall physiologic reserve rather than protein intake alone. Because albumin turns over slowly, a nutritional cause typically takes weeks to develop and weeks to correct, unlike some faster-changing markers.
सूजन संबंधी कारण
Perhaps the most clinically important nuance is that albumin behaves as a negative acute-phase reactant, meaning the liver deliberately reduces its production during significant inflammation and redirects resources toward other defensive proteins. Chronic inflammatory conditions, active infections, recent surgery, and critical illness can all suppress albumin independent of nutritional status, which is why a single low value should never be read as malnutrition alone. This is precisely why many labs now report albumin together with an inflammation marker; pairing a low albumin result with a CRP (C-reactive protein) test that is also elevated points toward inflammation rather than diet as the leading explanation.
| वर्ग | सामान्य कारणों में | Typical accompanying clues |
|---|---|---|
| जिगर | Cirrhosis, chronic hepatitis, fatty liver disease | Elevated AST/ALT, jaundice, fatigue |
| Kidney | Nephrotic syndrome, chronic kidney disease | Foamy urine, swelling, elevated urine albumin-to-creatinine ratio |
| पोषण | Malnutrition, malabsorption, restrictive diets | Weight loss, low prealbumin, muscle wasting |
| सूजन | Infection, surgery, chronic inflammatory disease, critical illness | Elevated CRP, fever, recent hospitalization |
| Dehydration/hemoconcentration (high albumin) | Fluid loss, inadequate fluid intake | Thirst, reduced urination, elevated total protein |
Causes of high albumin and dehydration
Elevated albumin, called hyperalbuminemia, is far less common than a low result and rarely reflects a disease process on its own. The leading explanation is dehydration, since a reduced fluid volume concentrates every protein in the blood, including albumin, making the level appear artificially high. Severe diarrhea, inadequate fluid intake, excessive diuretic use, and prolonged vomiting are frequent contributors. Rehydration typically brings the value back into range within days, and your doctor may simply recommend a repeat test after you have replenished fluids rather than pursuing an extensive workup.
A less common contributor is a diet very high in protein combined with reduced fluid intake, which can produce a mild, temporary elevation without any underlying illness. If a high albumin result repeats after adequate rehydration, your provider will look more broadly at kidney function and medication use before considering it a lasting pattern.
Albumin, total protein, and the albumin-to-globulin ratio
Albumin rarely stands alone on a lab report. Total protein reflects the combined concentration of albumin and a second family of proteins called globulins, which include antibodies and various transport molecules. Dividing albumin by globulin produces the albumin-to-globulin ratio, a quick screening figure that helps clinicians decide whether an abnormal total protein result stems mainly from the albumin side or the globulin side.
A falling albumin-to-globulin ratio often points toward liver disease, kidney protein loss, or a rise in globulins from chronic infection or an immune condition. A rising ratio is less common and can reflect reduced globulin production or concentrated albumin from dehydration. Because these three values interact so closely, many people find it helpful to review their total proteins blood test results alongside albumin, and to check their albumin-to-globulin ratio whenever a lab report includes it, since this combination gives a more complete view than any single figure in isolation.
How albumin compares with prealbumin as a nutrition marker
Laboratories sometimes measure a separate, faster-turnover protein alongside or instead of albumin when assessing nutrition specifically. You can review the details in our dedicated guide to prealbumin levels and transthyretin, but the key practical difference is timing: albumin has a half-life of roughly three weeks, so it reflects your protein status over the preceding month, while prealbumin turns over in only two to three days and reacts to changes in intake far more quickly.
This makes prealbumin more useful for tracking a nutrition intervention over days to weeks, while albumin remains the more established marker for longer-term liver, kidney, and overall physiologic assessment. Both proteins share the same inflammatory blind spot: acute illness suppresses each of them regardless of how well a person is eating, so clinicians typically interpret either result alongside a marker like CRP.
When to see a doctor about your albumin result
Most isolated, mildly abnormal albumin results do not require urgent action, but certain patterns deserve a prompt conversation with your healthcare provider.
- Seek care within a few days if you notice new or worsening swelling in your legs, ankles, or abdomen alongside a low albumin result.
- Schedule an appointment soon if unexplained fatigue, unintentional weight loss, or foamy urine accompanies an abnormal reading.
- Ask about follow-up testing if your albumin has fallen significantly compared with a previous result, even if the new value is still technically within range.
- Mention any recent surgery, infection, or hospitalization, since these can temporarily lower albumin through inflammation rather than a chronic disease.
- Discuss hydration and medication use if your albumin came back high, since this pattern is usually benign and reversible.
Simple monitoring, such as a repeat test in one to three months, is often appropriate when a mildly low value appears in isolation without symptoms or other abnormal markers.
How albumin is used alongside other lab panels
Clinicians rarely interpret albumin in isolation. It typically appears within a comprehensive metabolic panel or a dedicated liver function panel, where it sits next to markers such as liver enzymes, alkaline phosphatase, bilirubin, and total protein. When kidney disease is suspected, providers pair albumin with क्रिएटिनिन, eGFR, and a urine albumin-to-creatinine ratio to determine whether the kidneys are filtering properly or leaking protein. When inflammation or malnutrition is the leading concern, a CRP-to-albumin ratio or a nutrition-focused marker like prealbumin adds useful context that albumin alone cannot provide.
The table below offers a simplified way to think through a first-pass interpretation, though your provider will always weigh your full history and symptoms rather than relying on any single cutoff.
| Your albumin pattern | Helpful next check | इससे क्या संकेत मिल सकता है |
|---|---|---|
| Low albumin with elevated liver enzymes | Full liver panel, imaging if persistent | Reduced synthetic capacity from liver disease |
| Low albumin with foamy urine or swelling | Urine albumin-to-creatinine ratio, eGFR | Protein loss through the kidneys |
| Low albumin with elevated CRP | Clinical history for infection, surgery, or flare | Inflammation suppressing production, not diet |
| Low albumin with weight loss and low prealbumin | Dietary history, nutrition assessment | Genuine nutritional shortfall |
| High albumin with thirst or reduced urination | Hydration status, repeat test after fluids | Dehydration concentrating the result |
Recent scientific advances
Albumin research has moved well beyond its traditional role as a simple nutrition marker, and several recent studies help explain why doctors now treat it as a broader health signal rather than a stand-alone protein count.
A 2023 review found that lower albumin levels are linked to worse outcomes across a strikingly wide range of hospital settings, from heart disease to kidney conditions to cancer care. What this means for you: a low albumin result during a hospital stay is best understood as a general marker of how much physiological stress your body is under, not necessarily a sign that you are undernourished. In plain terms, albumin acts as a negative acute-phase reactant, meaning the liver purposefully makes less of it while fighting inflammation and redirects resources elsewhere. According to PubMed and Consensus, this pattern held consistently across cardiology, nephrology, oncology, and infectious disease settings (Gremese et al., 2023, Journal of Clinical Medicine).
A large 2024 analysis of stroke registry data, combined with a systematic review and meta-analysis, found that both unusually low and unusually high albumin levels at hospital admission were associated with a greater chance of long-term complications after a stroke. What this means for you: this is one more piece of evidence that albumin works best as a general marker for your doctor to weigh alongside your full clinical picture, rather than a number to interpret alone. The researchers used a restricted cubic spline model, a statistical method for detecting curved rather than straight-line relationships, which showed the pattern was not simply “lower is always worse” but instead formed a U-shaped curve (Thuemmler et al., 2024, Nutrients).
A 2025 study of nearly 2,800 hospitalized older adults compared the CRP-to-albumin ratio, which combines an inflammation marker with albumin, against another nutrition score for predicting early outcomes. What this means for you: combining albumin with an inflammation marker like CRP gives a more complete signal than either test alone, which is part of why your doctor may order both together, especially during a hospital stay. The combined ratio proved especially useful for identifying risk within the first week of a hospital admission, while the separate nutrition score performed better for assessments made over a longer stay (Capurso et al., 2025, Nutrients).
Taken together, this research reinforces a reassuring point for most people reviewing a routine result: a single albumin value outside the reference range, especially without symptoms, is rarely an emergency. It is a starting clue that your doctor will weigh alongside your history, symptoms, and other tests, and the growing use of combined markers like the CRP-to-albumin ratio reflects a broader shift toward interpreting results in context rather than in isolation.
शब्दकोष
| अवधि | Plain-language explanation |
|---|---|
| एल्बुमिन | The most abundant protein in blood plasma, made by the liver, that helps hold fluid in blood vessels and carry substances through the body. |
| हाइपोएल्ब्यूमिनमिया | The medical term for an albumin level below the normal reference range. |
| Hyperalbuminemia | The medical term for an albumin level above the normal reference range, most often caused by dehydration. |
| Negative acute-phase reactant | A substance, like albumin, whose production the liver reduces during inflammation or acute illness, regardless of nutritional status. |
| Oncotic pressure | The pulling force that proteins like albumin create to keep fluid inside blood vessels instead of leaking into tissue. |
| कुल प्रोटीन | The combined measurement of albumin and globulins in a blood sample. |
| Albumin-to-globulin ratio (A/G ratio) | A calculated figure comparing albumin to globulin levels, used to help narrow down the cause of an abnormal total protein result. |
| Prealbumin (transthyretin) | A separate, faster-turnover protein sometimes tested alongside albumin to track short-term changes in nutritional status. |
| नेफ़्रोटिक सिंड्रोम | A kidney condition that allows large amounts of albumin to leak from the blood into the urine. |
| सी-रिएक्टिव प्रोटीन (सीआरपी) | A separate blood marker that rises during inflammation and is often reviewed together with albumin. |
अक्सर पूछे जाने वाले प्रश्नों
Can certain medications change my albumin blood test result?
Yes. Corticosteroids and anabolic steroids can raise albumin production, while some medications bind tightly to the protein and can affect how a level is measured or interpreted. Insulin and certain hormone therapies have also been linked to modest changes. Because of this, it is worth telling your healthcare provider about every prescription, supplement, and over-the-counter medication you take before they interpret your result.
Does a low albumin level always mean poor nutrition?
No, and this is one of the more common misunderstandings about this test. Inflammation, infection, recent surgery, and liver or kidney disease can all lower albumin even when someone is eating adequately. Doctors typically look at markers like CRP alongside albumin, and sometimes add prealbumin, to separate a nutritional cause from an inflammatory one.
How does the albumin blood test relate to kidney function?
Two different tests use the word albumin in kidney care, and it helps to keep them distinct. This blood test measures albumin circulating in your bloodstream, while a separate urine test, the albumin-to-creatinine ratio, checks whether albumin is leaking into your urine. Healthy kidneys keep albumin in the blood and out of the urine, so finding albumin in urine, called albuminuria, is often an early sign of kidney damage, while a falling blood level can indicate heavier ongoing protein loss.
Can pregnancy affect a normal albumin blood test result?
Yes. Blood volume expands considerably during pregnancy, which naturally dilutes albumin and produces a gradual, expected decline, particularly by the third trimester. A sudden or more pronounced drop is different from this expected pattern and warrants prompt evaluation, since it can occasionally signal a complication such as preeclampsia.
Why did my albumin come back slightly outside the reference range with no symptoms at all?
A mildly abnormal result without symptoms is common and often reflects a temporary factor such as recent illness, hydration status, or normal variation between laboratories. Many healthcare providers recommend simply repeating the test after a defined interval to see whether the value normalizes before pursuing further investigation.
Is fasting required before an albumin blood test?
Typically not. Albumin levels are not meaningfully affected by a recent meal, so fasting is not usually required specifically for this test. However, if your blood draw includes other tests that do require fasting, such as a glucose or lipid panel, your provider may ask you to fast for the full visit.
सूत्रों का कहना है
- MedlinePlus (National Library of Medicine, NIH) — Albumin Blood Test, 2024 — link
- Cleveland Clinic — Albumin Blood Test, 2024 — link
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK, NIH) — Albuminuria: Albumin in the Urine, 2016 — link
- Gremese E, et al. — Serum Albumin Levels: A Biomarker to Be Repurposed in Different Disease Settings in Clinical Practice — Journal of Clinical Medicine, 2023 — link
- Thuemmler R, et al. — Serum Albumin and Post-Stroke Outcomes: Analysis of UK Regional Registry Data, Systematic Review, and Meta-Analysis — Nutrients, 2024 — link
- Capurso C, et al. — C-Reactive Protein/Albumin Ratio vs. Prognostic Nutritional Index as the Best Predictor of Early Mortality in Hospitalized Older Patients — Nutrients, 2025 — link
अग्रिम पठन
- BUN (Urea): understanding your test results
- एल्कलाइन फॉस्फेटेज (ALP) परीक्षण: अपने परिणामों को समझना
- फेरिटिन: आपके स्वास्थ्य के लिए इस रक्त मार्कर को समझना
- Urine creatinine levels: guide and interpretation
- Vitamin B12: understanding its role and your lab results
Albumin rarely tells the full story on its own, and pairing it with related results such as total protein, prealbumin, creatinine, and CRP often clarifies what a single abnormal value means. Reviewing several markers together, rather than fixating on one line of a report, is exactly the kind of pattern that becomes easier to see with structured support. AI DiagMe helps you understand these connections across your own lab results, without offering a diagnosis or replacing the judgment of your doctor.
AI DiagMe की मदद से अपने लैब परिणामों को समझें
कुछ ही मिनटों में अपने परिणामों का विश्लेषण प्राप्त करें
{kind=link}