














Direct bilirubin is the fraction of bilirubin your liver has already processed and prepared for elimination through bile. When this value sits above the reference range on a lab report, it usually points toward the liver or bile ducts rather than a red blood cell problem. This guide explains what direct bilirubin measures, how it differs from indirect and total bilirubin, what a high or low result can mean, and which questions are worth bringing to a follow-up visit. The goal is a clear, factual starting point you can use alongside your doctor’s advice, not a replacement for it.
What direct bilirubin is and where it comes from
Bilirubin begins as a byproduct of old red blood cells. After roughly 120 days in circulation, red blood cells break down, mostly inside the spleen. This process releases hemoglobin, which is converted into a yellow-orange pigment called indirect (or unconjugated) bilirubin. Because this initial form does not dissolve in water, it must travel through the bloodstream attached to a protein called albumin.
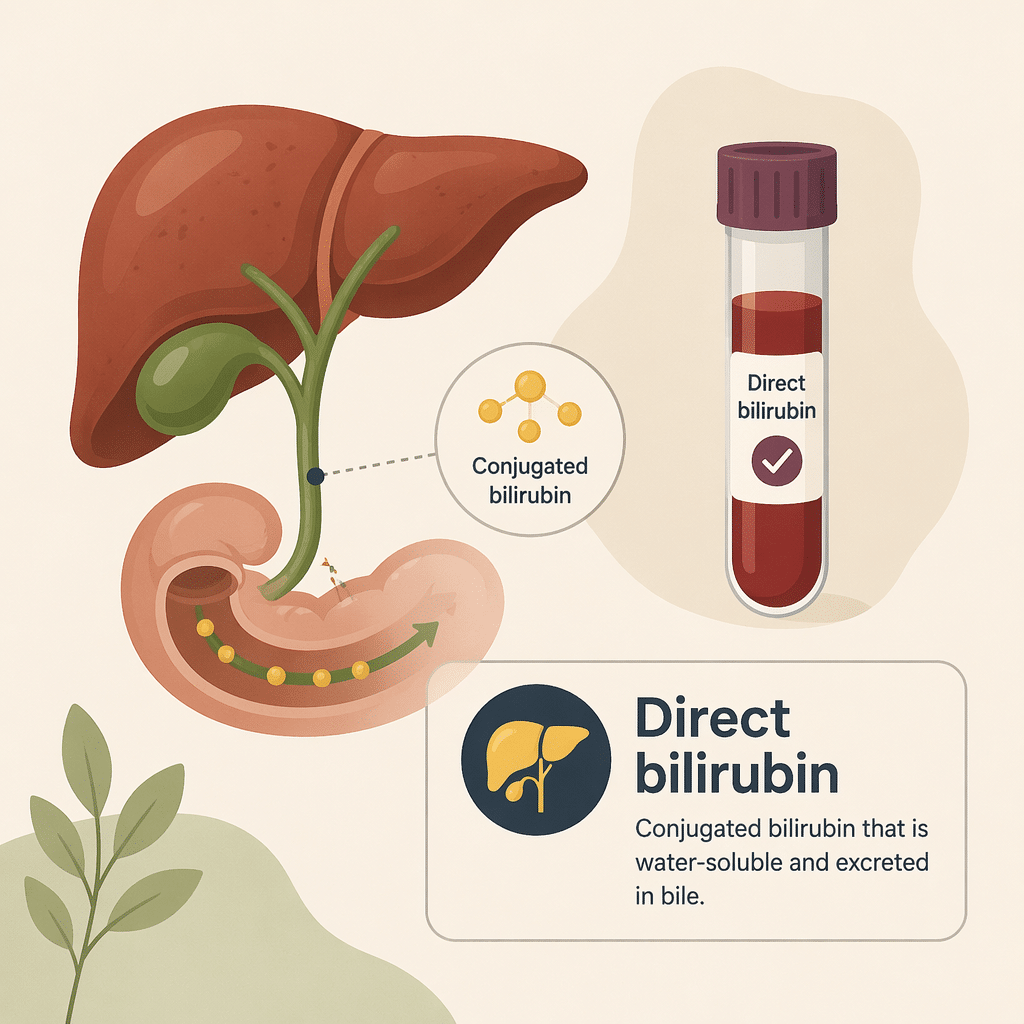
The liver takes over from there. Liver cells attach a sugar molecule called glucuronic acid to indirect bilirubin, a step chemists call conjugation. Once conjugated, the pigment becomes water-soluble and picks up a new name: direct bilirubin. This transformed form can then be released into bile, carried into the intestine, and eventually removed from the body in stool, which is what gives stool its typical brown color.
Why the liver bothers to convert it
Conjugation exists because the body needs a way to safely package and excrete a substance that would otherwise build up in tissues. A functioning liver converts indirect bilirubin efficiently, so only a small amount of direct bilirubin should ever appear in the blood at any given time. When more of it accumulates than normal, that signals either a bile flow problem or liver cell dysfunction rather than excess pigment production.
Direct bilirubin versus indirect and total bilirubin
Lab reports for liver function typically show three related bilirubin values together, and understanding how they interact matters more than looking at any single number in isolation.
- Clinicians also track total bilirubin levels, which combine both fractions and give an overall picture.
- Direct (conjugated) bilirubin reflects what the liver has already processed.
- Indirect (unconjugated) bilirubin is calculated by subtracting direct bilirubin from the total.
Clinicians use the pattern among these three values, together with related enzymes, to interpret a full liver function tests panel and distinguish between different categories of disease. An isolated rise in indirect bilirubin often points toward increased red blood cell breakdown or a mild inherited conjugation issue such as Gilbert syndrome. A predominant rise in direct bilirubin instead points toward the liver or bile ducts, which is the focus of this article.
Normal direct bilirubin ranges
Reference ranges vary slightly between laboratories depending on the equipment and method each lab uses, so always check the range printed next to your own result. As a general guide, most adult laboratories consider a direct bilirubin level below 0.3 mg/dL (about 5.1 micromoles per liter) to fall within the normal range. Direct bilirubin normally makes up a small share, typically well under a quarter, of the total bilirubin value.
Age and sex have little effect on adult reference ranges. The main exception involves newborns, whose still-maturing livers can struggle to conjugate bilirubin efficiently, which is why infant jaundice is closely monitored in the first days of life using different reference thresholds than those used for adults.
What a high direct bilirubin level can mean
An elevated direct bilirubin result tells your clinician that conjugation itself is working, since the pigment has already been processed, but that something is interfering with its excretion into bile or its clearance from the bloodstream. Causes generally fall into two broad categories: problems affecting bile flow, often called cholestatic or obstructive, and problems affecting liver cells directly, often called hepatocellular.
Bile duct and bile flow causes
When bile cannot move freely from the liver to the intestine, conjugated bilirubin backs up into the bloodstream. Common causes include gallstones blocking a duct, inflammation of the bile ducts known as cholangitis, and tumors of the pancreas or bile ducts that press on the drainage pathway. These conditions often raise alkaline phosphatase test results and elevate gamma-glutamyl transferase readings alongside direct bilirubin, and they frequently produce dark urine and pale, clay-colored stools because less bilirubin reaches the intestine.
Liver cell causes
Damage or inflammation inside liver cells can also impair the release of conjugated bilirubin into bile, even without a physical blockage. Autoimmune and drug-induced hepatitis are common examples, and clinicians also rule out viral causes by ordering markers such as HBs antigen for hepatitis B ja anti-HCV for hepatitis C, alongside cirrhosis screening. In these situations, clinicians watch AST test results ja ALT levels for a sharper rise than alkaline phosphatase, which helps a clinician judge whether the liver cells themselves or the drainage system is the primary problem.
Harvinaisempia syitä
A small number of inherited conditions, including Dubin-Johnson syndrome and Rotor syndrome, impair the liver’s ability to transport already-conjugated bilirubin into bile. These conditions are generally benign and do not progress to serious liver disease, though they still require a proper diagnosis to rule out more concerning explanations for elevated direct bilirubin.
Hepatocellular versus cholestatic patterns: a quick comparison
The table below summarizes how clinicians typically distinguish these two broad patterns when direct bilirubin is elevated. This is a general guide, not a diagnostic tool, and your own results always need interpretation in the context of your full clinical picture.
| Ominaisuus | Cholestatic (bile flow) pattern | Hepatocellular (liver cell) pattern |
|---|---|---|
| Alkalinen fosfataasi (ALP) | Markedly elevated | Normal or mildly elevated |
| AST and ALT | Normal or mildly elevated | Markedly elevated |
| Tyypilliset oireet | Itching, pale stools, dark urine | Fatigue, nausea, right upper abdominal discomfort |
| Yleisiä esimerkkejä | Gallstones, cholangitis, tumors compressing bile ducts | Viral or autoimmune hepatitis, cirrhosis, drug-induced liver injury |
| Tavallinen seuraava vaihe | Abdominal ultrasound or MRCP | Viral hepatitis panel and medication review |
Related symptoms to watch for
Because direct bilirubin is water-soluble, elevated levels can spill into urine and reduce the amount reaching the intestine, which produces a recognizable set of symptoms.
- Jaundice, a yellowing of the skin and the whites of the eyes.
- Tumma, teenvärinen virtsa.
- Vaalea tai savenvärinen uloste.
- Itching, which can occur when bile salts build up in the skin.
- Right upper abdominal discomfort, particularly with gallstone-related causes.
Fatigue and loss of appetite can accompany any of these causes, but they are nonspecific and appear in many unrelated conditions, so they are not reliable indicators on their own.
Milloin mennä lääkäriin
Contact your doctor promptly if you notice yellowing of the skin or eyes, unusually dark urine, pale stools, or persistent right upper abdominal pain. Seek urgent care if these symptoms occur together with fever, confusion, or severe pain, since this combination can indicate a bile duct infection that needs prompt treatment. For a mild, isolated elevation without symptoms, a routine follow-up visit to repeat the test and check trends is usually the appropriate first step, and your doctor will decide whether imaging or additional blood work is needed based on the pattern of your results.
Recent scientific advances
Bilirubin research has moved beyond viewing this pigment as simple metabolic waste, and several recent analyses have sharpened how direct bilirubin measurements are used in practice.
A large 15-year birth cohort study from Utah, published in The Journal of Pediatrics, found that a fractionated bilirubin test reliably flagged infants who later turned out to have biliary atresia, a serious blockage of the bile ducts (Kastenberg et al., 2023). What this means for you: while that study focused on newborn screening rather than adult testing, it reinforces a broader principle that also applies to adults, namely that direct bilirubin is a highly sensitive marker for bile flow problems, which is why doctors lean on it so heavily when investigating jaundice at any age. Fractionated bilirubin, in plain terms, simply means bilirubin broken down into its direct and indirect components rather than reported only as a single total number.
A related systematic review and meta-analysis pooling data from more than 1.8 million newborns found that direct or conjugated bilirubin testing performed with very high accuracy for identifying bile duct blockages, outperforming other screening approaches such as stool color checks alone (Gopal et al., 2024, PLOS ONE). What this means for you: this large body of evidence is part of why an elevated direct bilirubin result is treated as a meaningful signal that warrants investigation rather than something to dismiss, even though the specific studies were conducted in infants. Biliary atresia itself is a pediatric condition, but the diagnostic logic, that direct bilirubin points reliably toward bile duct dysfunction rather than red blood cell turnover, is the same principle clinicians apply when evaluating adults with an unexplained rise in this marker.
Taken together, this growing evidence base supports what clinical practice has long assumed: direct bilirubin is not just a number to note in passing, but one of the more dependable clues for narrowing down whether a bile flow problem or a liver cell problem is driving an abnormal result. None of this research suggests reason for alarm about a single test result; it instead explains why your doctor takes this particular marker seriously and why prompt follow-up on a significant elevation is worthwhile.
Sanasto
| Termi | Merkitys |
|---|---|
| Conjugated bilirubin | Another name for direct bilirubin, referring to bilirubin that the liver has chemically modified to make it water-soluble. |
| Unconjugated bilirubin | Another name for indirect bilirubin, the form that has not yet been processed by the liver. |
| Cholestasis | A slowdown or blockage of bile flow from the liver to the intestine, one of the main causes of elevated direct bilirubin. |
| Keltatauti | Yellowing of the skin and eyes that occurs when bilirubin builds up in the blood and tissues. |
| Hepatocellular | Relating to liver cells directly, as opposed to the bile ducts that carry bile away from the liver. |
| Alkalinen fosfataasi (ALP) | An enzyme from the liver and bones that rises prominently when bile flow is blocked. |
| Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) | Two liver enzymes that rise mainly when liver cells themselves are injured or inflamed. |
| Biliary atresia | A rare, serious blockage of the bile ducts that affects newborns and is often detected through fractionated bilirubin screening. |
Usein kysytyt kysymykset
Can medications raise direct bilirubin levels?
Yes. Certain antibiotics, including amoxicillin-clavulanate, along with some anti-inflammatory drugs and antiretroviral medications, can affect bile flow and raise direct bilirubin, a pattern sometimes called drug-induced cholestasis. This effect is usually reversible once the medication is stopped, but any change should be discussed with the prescribing doctor rather than adjusted on your own. Always share a complete medication and supplement list with your doctor when reviewing an abnormal result.
How is a bile duct problem told apart from a liver cell problem?
Clinicians look at the overall pattern across the liver panel rather than direct bilirubin in isolation. A bile duct obstruction typically raises alkaline phosphatase and direct bilirubin together, while a liver cell problem such as hepatitis typically raises AST and ALT more prominently. Imaging, usually an abdominal ultrasound, often confirms which pattern is present.
Does direct bilirubin change with fasting or exercise?
Prolonged fasting can raise total bilirubin slightly, though this effect mainly involves the indirect fraction rather than direct bilirubin. Intense exercise can transiently affect liver enzymes more broadly. Most labs suggest avoiding extended fasting and strenuous activity for about a day before a blood draw to get the most representative baseline result.
Is a high direct bilirubin level after surgery something to worry about?
A temporary rise in direct bilirubin is common in the days following abdominal surgery, particularly procedures involving the liver or bile ducts, and often reflects post-operative inflammation or anesthesia effects rather than a new complication. Levels typically settle within one to two weeks. A persistent or worsening elevation warrants follow-up with the surgical team.
Do direct bilirubin reference ranges change with age?
In adults, reference ranges stay fairly stable across age groups and between sexes. The clearest exception is the newborn period, when an immature liver conjugates bilirubin more slowly, which is why infants are screened using separate, age-specific thresholds rather than adult reference ranges.
What does a normal direct bilirubin with a high total bilirubin usually mean?
This combination points toward the indirect fraction rather than the liver’s drainage system, since the direct portion is normal. Possible explanations include increased red blood cell breakdown, called hemolysis, or a mild inherited conjugation issue such as Gilbert syndrome. Your doctor will typically order additional tests targeted at red blood cell health to clarify the cause.
Lähteet
- Kastenberg ZJ, et al. — Fractionated Bilirubin Among 252,892 Utah Newborns with and Without Biliary Atresia: A 15-year Historical Birth Cohort Study — The Journal of Pediatrics, 2023 — https://doi.org/10.1016/j.jpeds.2022.12.041
- Gopal SH, et al. — Population-based screening strategies for biliary atresia in the newborn: A systematic review and meta-analysis — PLOS ONE, 2024 — https://consensus.app/papers/details/5c09cd3963b65b3795a7f32351d5c39a/
- National Library of Medicine (MedlinePlus) — Bilirubin Blood Test — U.S. National Institutes of Health, 2024 — https://medlineplus.gov/lab-tests/bilirubin-blood-test/
- Mayo Clinic Staff — Bilirubin blood test — Mayo Clinic, 2026 — https://www.mayoclinic.org/tests-procedures/bilirubin/about/pac-20393041
- Cleveland Clinic — Bilirubin Test: Understanding High vs. Low Levels & Causes — Cleveland Clinic, 2023 — https://my.clevelandclinic.org/health/diagnostics/17845-bilirubin
Lisälukemista
- Kokonaisbilirubiinitasot: täydellinen oppaasi tähän tärkeään markkeriin
- AST-normaalialue: tasojen ja syiden ymmärtäminen
- ALT-tasot: Merkitys, syyt ja normaalialueet -opas
- Gammaglutamyylitransferaasi (GGT): Täydellinen opas tähän maksaentsyymiin
- Alkalisen fosfataasin (ALP) testi: tulosten ymmärtäminen
Direct bilirubin rarely tells the whole story on its own, and comparing it against related markers often clarifies what is happening far more than any single value. Reviewing a full gamma-glutamyl transferase and liver panel result set together, alongside symptoms like jaundice or changes in urine and stool color, gives a clearer picture of whether bile flow or liver cells need closer attention. AI DiagMe helps you understand what your lab results are showing in plain language, so you arrive at your next doctor’s visit with clearer questions. It does not diagnose conditions or replace your doctor’s judgment, but it can make the numbers on your report far less intimidating.
Ymmärrä laboratoriotuloksiasi tekoälyn DiagMen avulla
Tulkitse tuloksesi muutamassa minuutissa

{kind=link}